Background: Clonidine is an α-adrenoreceptor agonist that reduces sympathetic outflow and releases certain neurotransmitters by acting on receptors in the brain and peripheral tissues. The aim of this systematic review and meta-analysis is about the effectiveness and safety of clonidine for controlling blood loss, hemodynamic stability and surgical field quality comparing with tranxemic acid, placebo and dexmedetomidine. The randomized controlled trials that determine the effect of clonidine on blood loss, hemodynamic stability, and surgical field quality in adult patients undergoing oral and maxillofacial surgery were included. The articles included in this systematic review were searched through the electronic databases PubMed, Cochrane Library, and Google Scholar from July to September 17, 2025. The primary outcomes were controlling blood loss, hemodynamic stability, and surgical field quality. Secondary outcomes were duration of surgery and adverse events. The risk of bias was assessed by the Cochrane Collaboration tool (ROB2). Subgroup and sensitivity analysis was conducted to investigate the study of high risk of bias. Mean difference and relative risk with a 95% confidence interval were used for analysis. There were 15 articles included in the review after screening 615, with a total population of 1143. Clonidine was less blood loss than tranxemic acid (MD=40.17, 95% CI: 4.95- 75.38; p=0.03), more blood loss control than with placebo (MD=-75.15, 95% CI: -96.04-54.25; p <0.00001), and less blood loss control than with dexmedetomidine (MD=7.65, 95% CI: 1.19-14.11; p=0.02). Clonidine maintained mean arterial blood pressure than placebo (MD = -3.87, 95% CI: -6.01--1.72; p = 0.0004). Clonidine is maintained MAP in normal range than placebo when administered Pre-induction (MD=-1.88,95% CI: -3.7--0.07; p=0.04) compared with post induction (MD = -8.16.95% CI: -13.7--2.62; p=0.004). Clonidine has less poor and fair surgical field quality than placebo (RR=0.1, 95% CI: 0.02-0.42, p=0.002; RR=0.82, 95% CI: 0.67-1, p=0.05) respectively. Clonidine decreases blood loss more than placebo. Clonidine is less likely inferior to dexmedetomidine to reducing blood loss for oral and maxillofacial surgery. Clonidine maintains mean arterial blood pressure in the normal range than placebo when administered pre-induction than after induction. Clonidine maintains MAP before induction, and it is effective pre-induction as well as post-induction to maintain a mean heart rate comparable with dexmedetomidine. Clonidine is shortening the duration of surgery comparably with tranxemic acid and dexmedetomidine but more than placebo.
| Published in | Science Discovery Medicine (Volume 1, Issue 2) |
| DOI | 10.11648/j.sdmed.20260102.12 |
| Page(s) | 62-78 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Blood Loss, Clonidine, Effectiveness, Hemodynamic, Surgical Field Quality
Author | Year | Area | study design | S. size | Intervention | Main outcome |
|---|---|---|---|---|---|---|
Jan et. al | 2014 | India | RCT | 120 | Oral clonidine 5 mcg/kg vs famotidine 40mg | oral clonidine reduce bleeding in endoscopic sinus surgery |
Khandelwal et al | 2023 | India | RCT | 60 | Clonidine 200 mcg 60 minute before surgery vs sip water before 60 minutes | Pre-emptive clonidine reduces surgical bleeding by controlling haemodynamic in FSS |
Arafat et al | 2024 | Egypt | RCT | 40 | 2 mcg oral clonidine taken 1 to 1.5 hours before operation | Premedication of oral clonidine improves hemodynamic status, surgical field, decrease blood loss |
M. B. Heydari, M. Safdari, B. Hmmatopoor | 2024 | Iran | RCT | 92 | TXA 700mg/kg 2 hours before surgery and Oral clonidine 2mcg/kg 90 minute before surgery | Use of TXA compared with clonidine more control of bleeding in Rhinoplasty |
Von et al | 2024 | Egypt | RCT | 80 | 3mcg/kg clonidine diluted in 10 ml 0.9% NS followed by infusion 0.4mcg/kg /hr vs 1mcg/kg Dex diluted in 10ml of 0.9%NS followed by infusion of 0.4mcg/kg/hr | both dexmedetomidine and clonidine good to excellent surgical field visuality, blood loss and duration of surgery are comparable |
suggala kk. et al | 2020 | India | RCT | 60 | 3mcg/kg of clonidine in diluted of 10ml of 0.9%NS infused over 10 minutes before induction followed by infusion vs 1mcg/kg of Dex. diluted in 10 ml 0.9% NS 10 minute before induction followed by infusion 0.4-0.8 mcg | Clonidine is used as hemodynamic stability, safe operative field Visuality, decreased blood loss |
Krishna et al | 2025 | India | RCT | 80 | 3mcg/kg of clonidine diluted of 100ml of 0.9%NS given 15 minute before induction vs 1mcg/kg of Dex. Diluted in 100ml of 0.9% NS given 15 minutes before induction | controlled hypotension were achieved with either Dex. or clonidine, Dex. has better haemodynamic stability, decreased blood loss, and excellent surgical field visuality than Clonidine |
D, V. Praven. et al | 2024 | India | RCT | 80 | 1mcg/kg of Dex. given over period of 10 minute before induction followed by infusion of 0.2-0.7 mcg/ kg/hr vs 2mcg/kg of clonidine given 10 minutes of 1-2 mcg/kg/hr | Controlled hypotension, intraoperative blood loss, better surgical field vision, and postoperative recovery |
Bafna et al | 2021 | India | RCT | 70 | 1mcg/kg of Dex. Diluted in 10ml given over period of 10 minute before induction and followed by infusion 1mcg/kg/hr vs 2mcg/kg of clonidine diluted induction followed by infusion of 1mcg/kg/hr | both dexmedetomidine and clonidine for controlled hypo tension to improve surgical field quality. Dex. provide more hemodynamic stability and postoperative analgesia than Clonidine |
Das et al | 2016 | India | RCT | 66 | IV Dex 1mcg/kg diluted in Saline given 15 minutes before induction vs IV clonidine 1.5 mcg/kg diluted in 100ml saline given 15 minutes before induction | Dexmedetomidine is more effective than clonidine in controlled hypotension, less blood loss, more surgical field quality and analgesia |
Ghorbani J et al | 2018 | Iran | RCT | 52 | IV TXA 15nl/kg diluted in 100ml NS was given and followed by infusion 10 minute after induction vs 0.2 mg oral clonidine was given 1 to 1.5 hours before surgery by infusion | bleeding control, surgical field visualization and surgical satisfaction |
Akram Hammatpoor et al | 2023 | Iran | RCT | 120 | 3mcg/kg of clonidine given oraly 90 minute before surgery vs 250 mcg/kg TXA orally before 2 hours | Clonidine more effective of bleeding than TXA |
Jabalameli et al | 2005 | Iran | RCT | 113 | 5 mcg/kg of clonidine received 90 minutes before operation | Premedication with oral clonidine reducing bleeding and controlled hypotension with fentanyl and hydralazine for controlled hypotension |
Suman Kaushik et al | 2019 | India | RCT | 50 | 20 ml of normal saline in premedication vs 3mcg/kg body weight in 20 ml normal saline | clonidine is cheap and safe drug for controlled hypotension |
Jiwanmall et al | 2017 | India | RCT | 60 | 3mcg/kg of clonidine vs sterile water was given 30 minutes before induction | clonidine is reduce intraoperative blood loss, additional hypotensive drugs, improve surgical field quality and good analgesia |
Author | Study design | Risk of bias | Inconsistency | Indirectness | Impression | Publication bias | Level of quality |
|---|---|---|---|---|---|---|---|
Jan et. al 2014 | RCT | Not serious | Not serious | Not serious | Not serious | Undetected | High |
Khandelwal et al 2023 | RCT | Not serious | Not serious | Serious | Not serious | Suspected | Moderate |
Arafat et al 2024 | RCT | Not serious | Not serious | Not serious | Not serious | Undetected | High |
M. B. Heydari, M. Safdari 2024 | RCT | Not serious | Serious | Not serious | Not serious | Undetected | Low |
Von et al 2024 | RCT | Not serious | Not serious | Not serious | Not serious | Suspected | Moderate |
suggala kk. et al 2020 | RCT | Not serious | Not serious | Serious | Not serious | Not suspected | Moderate |
Krishna et al 2025 | RCT | Not serious | Not serious | Serious | Not serious | Suspected | Moderate |
D, V. Praven. et al 2024 | RCT | Not serious | Not serious | Serious | Not serious | Undetected | Moderate |
Bafna et al 2021 | RCT | Not serious | Not serious | Serious | Not serious | Undetected | Moderate |
Das et al 2016 | RCT | Not serious | Not serious | Serious | Not serious | Suspected | Moderate |
Ghorbani J et al 2018 | RCT | Not serious | Not serious | Not serious | Not serious | Undetected | High |
Akram Hemmatpoor 2023 | RCT | Serious | Serious | Not serious | Not serious | Suspected | Low |
Jabalameli et al 2005 | RCT | Not serious | Not serious | Not serious | Not serious | Not suspected | High |
Suman Kaushik et al 2019 | RCT | Not serious | Not serious | Not serious | Not serious | Not suspected | High |
Jiwanmall et al 2017 | RCT | Not serious | Not serious | Not serious | Not serious | Undetected | High |
Dex | Dexmedetomidine |
GRADE | Grade of Recommendation, Assessment, Development and Evaluation |
IV | Intravenous |
MAP | Mean Arterial Blood Pressure |
MD | Mean Difference |
MHR | Mean Heart Rate |
NS | Normal Saline |
PRISMA | Protocol of Systematic Review of Meta-Analysis |
PICO | Population, Intervention, Comparator, Outcome |
RR | Relative Risk |
RCT | Randomized Controlled Trial |
SRMA | Systematic Review and Meta-analysis |
TXA | Tranxemic Acid |
| [1] | D. Ommi, H. Teymourian, A. Zali, F. Ashrafi, and M. Jabbary, “Effects of Clonidine Premedication on Intraoperative Blood Loss in Patients With and Without Opium Addiction During Elective Femoral Fracture Surgeries,” vol. 5, no. 4, pp. 25–30, 2015, |
| [2] | F. Janatmakan, S. Nesioonpour, F. J. Zadeh, A. Teimouri, and M. Vaziri, “Comparing the Effect of Clonidine and Dexmedetomidine on Intraoperative Bleeding in Spine Surgery,” vol. 9, no. 1, pp. 1–5, 2019, |
| [3] | A. Shah, A. J. R. Palmer, and A. A. Klein, “Strategies to minimize intraoperative blood loss during major surgery,” Br. J. Surg., vol. 107, no. 2, pp. e26–e38, 2020, |
| [4] | A. Ebneshahidi and M. Mohseni, “Premedication with oral clonidine decreases intraoperative bleeding and provides hemodynamic stability in cesarean section,” vol. 1, no. 1, pp. 30–33, 2011, |
| [5] | S. Amna, J. V. Sigaard, and T. K. Bergmann, “Review of clinical pharmacokinetics and pharmacodynamics of clonidine as an adjunct to opioids in palliative care,” no. December 2023, pp. 485–497, 2024, |
| [6] | H. S. Fernandes, B. J. Sci, T. Res, H. S. Fernandes, S. A. Santos, and H. A. Ashmawi, “Clonidine in Anesthesiology : A Brief Review,” vol. 5, no. 4, pp. 5815–5818, 2018, |
| [7] | J. Ghorbani, S. Arastou, A. S. Naeini, and N. Raad, “Comparing the Effect of Oral Clonidine and Tranexamic Acid on Bleeding and Surgical Field Quality during Functional Endoscopic Sinus Surgery,” vol. 30, no. 100, 2018. |
| [8] | M. B. Heydari, M. Safdari, and B. Hemmatpoor, “Comparative Study of the Effects of Clonidine and Tranexamic Acid on Intraoperative Bleeding in Rhinoplasty : A Clinical Trial,” JPRAS Open, vol. 41, pp. 183–193, 2024, |
| [9] | Akraham Hemmatpor, C. Trial, “Comparing the Effect of oral Clonidine and Tranexamic Acid on Bleeding During Rhinoplasty Under General Anesthesia: 2023; 3(227): 50–61. Clinical Trials Registry Number: IRCT20121229011923N6. |
| [10] | M. Jan, F. A. Reshi, S. Gupta, S. Aara, I. H. Wani, and B. Saleem, “Evaluation of Oral Clonidine Premedication on Intraoperative Blood Loss and Bleeding Severity Score in Functional Endoscopic Sinus Surgery – A Prospective Placebo Controlled Study,” vol. 4, no. 10, pp. 1970–1979, 2014. |
| [11] | O. Article, “Intravenous clonidine as a part of balanced anaesthesia for controlled hypotension in functional endoscopic sinus surgery : A randomised controled trial,” no. 60, pp. 418–423, 2017. |
| [12] | S. Kaushik, H. Bamaniya, and Y. S. Chundawat, “Role of clonidine premedication as a part of hypotensive anaesthesia during functional endoscopic sinus surgery : A placebo-controlled study,” vol. 11, no. August, pp. 110–113, 2019. |
| [13] | M. Ragab, A. Mahmoud, R. Reda, and K. A. El, “The Effect of Oral Clonidine Premedication on the blood Loss and the Quality of Surgical Field during Endoscopic Sinus Surgery,” vol. 5, no. 2, 2024. |
| [14] | S. Arafat, A. Attia, and R. Ibrahim, “Bleeding Disorders In Oral And Maxillofacial Surgery And Management Guidelines,” vol. 24, no. 8, pp. 55–63, 2025, |
| [15] | K. Khandelwal and J. Sen, “A Study of the Effect of Pre-emptive Oral Clonidine on Intraoperative Haemodynamics and Surgical Field Quality During Functional Endoscopic Sinus Surgery Under General Anaesthesia,” vol. 15, no. 4, 2023, |
| [16] | O. Article, “Induced hypotension in ambulatory functional endoscopic sinus surgery : A comparison between dexmedetomidine and clonidine as premedication. A prospective, double-blind, and randomized study,” no. 1, 2016, |
| [17] | K. K. Suggala, B. K. Rao, and M. H. Nagrale, “Comparison of Dexmedetomidine, with Clonidine Based Anaesthesia for Controlled Hypotension in Functional Endoscopic Sinus Surgery,” vol. 7, no. 15, pp. 3–7, 2020, |
| [18] | O. Article, “Comparison of hypotensive properties of dexmedetomidine versus clonidine for induced hypotension during functional endoscopic sinus surgery : A randomised, double - blind interventional study,” no. 21, pp. 579–585, 2021. |
| [19] | E. N. Mugabo et al., “Clonidine and dexmedetomidine for controlled hypotension during functional endoscopic sinus surgery : a comparative study,” 2024. |
| [20] | D. V Praveen, K. Jayasudha, and S. R. Kumar, “Comparison of Dexmedetomidine, with Clonidine Based Anaesthesia for Controlled Hypotension in Functional Endoscopic Sinus Surgery,” vol. 18, no. 10, 2024, |
| [21] | J. A. C. Sterne et al., “RoB 2 : a revised tool for assessing risk of bias in randomised trials as an essential component of a,” pp. 1–8, |
| [22] | S. Krishna et al., “Comparison of the Efficacy of Intravenous Dexmedetomidine versus Intravenous Clonidine for Controlled Hypotension during Functional Endoscopic Sinus Surgery : A Prospective Observational Study,” pp. 1–6, 2025, |
| [23] |
D. Sir, “Clinical Epidemiology and Global Health,” vol. 5, no. January, pp. 0–1, 2016, [Online]. Available:
https://findit.dtu.dk/en/catalog/2397970748%0A http://www.journals.elsevier.com/clinical-epidemiology-and-global-health/recent-articles%5Cnhttp://files/241/recent-articles.html |
| [24] | M. Jabalameli, M. Hashemi, H. Soltani, and J. Hashemi, “Oral clonidine premedication decreases intraoperative bleeding in patients undergoing endoscopic sinus surgery,” J. Res. Med. Sci., vol. 10, no. 1, pp. 25–30, 2005. |
| [25] | Y. M. Lin, C. Yu, and G. Z. Xian, “Calculation methods for intraoperative blood loss: a literature review,” BMC Surg., vol. 24, no. 1, 2024, |
| [26] | S. Bhat and S. M. D. S. Periasamy, “Effectiveness of clonidine as a preanesthetic drug on intra operative blood loss in oral and maxillofacial surgery,” Int. J. Health Sci. (Qassim)., vol. 5, pp. 344–362, 2021, |
| [27] | Z. A. Varzaneh, A. Hemmatipour, and H. Kazemi-arpanahi, “Comparing the effect of pre- anesthesia clonidine and tranexamic acid on intraoperative bleeding volume in rhinoplasty : a machine learning approach,” pp. 1–13, 2025. |
| [28] | V. Erick et al., “parative study,” 2024. schienen in: BMC Anesthesiology | Ausgabe 1/2024. |
APA Style
Hordofa, T. A., Ilala, T. T., Feye, S. M., Nerso, K. M., Urji, D. T., et al. (2026). Effectiveness and Safety of Clonidine for Controlling Blood Loss, Hemodynamic Stability, and Surgical Field Quality in Oral and Maxillofacial Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Science Discovery Medicine, 1(2), 62-78. https://doi.org/10.11648/j.sdmed.20260102.12
ACS Style
Hordofa, T. A.; Ilala, T. T.; Feye, S. M.; Nerso, K. M.; Urji, D. T., et al. Effectiveness and Safety of Clonidine for Controlling Blood Loss, Hemodynamic Stability, and Surgical Field Quality in Oral and Maxillofacial Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sci. Discov. Med. 2026, 1(2), 62-78. doi: 10.11648/j.sdmed.20260102.12
AMA Style
Hordofa TA, Ilala TT, Feye SM, Nerso KM, Urji DT, et al. Effectiveness and Safety of Clonidine for Controlling Blood Loss, Hemodynamic Stability, and Surgical Field Quality in Oral and Maxillofacial Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Sci Discov Med. 2026;1(2):62-78. doi: 10.11648/j.sdmed.20260102.12
@article{10.11648/j.sdmed.20260102.12,
author = {Tesfaye Asefa Hordofa and Tajera Tageza Ilala and Simon Mengistu Feye and Kelil Musa Nerso and Dinku Tsegaye Urji and Ebrahim Ahmed Hussen},
title = {Effectiveness and Safety of Clonidine for Controlling Blood Loss, Hemodynamic Stability, and Surgical Field Quality in Oral and Maxillofacial Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials},
journal = {Science Discovery Medicine},
volume = {1},
number = {2},
pages = {62-78},
doi = {10.11648/j.sdmed.20260102.12},
url = {https://doi.org/10.11648/j.sdmed.20260102.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdmed.20260102.12},
abstract = {Background: Clonidine is an α-adrenoreceptor agonist that reduces sympathetic outflow and releases certain neurotransmitters by acting on receptors in the brain and peripheral tissues. The aim of this systematic review and meta-analysis is about the effectiveness and safety of clonidine for controlling blood loss, hemodynamic stability and surgical field quality comparing with tranxemic acid, placebo and dexmedetomidine. The randomized controlled trials that determine the effect of clonidine on blood loss, hemodynamic stability, and surgical field quality in adult patients undergoing oral and maxillofacial surgery were included. The articles included in this systematic review were searched through the electronic databases PubMed, Cochrane Library, and Google Scholar from July to September 17, 2025. The primary outcomes were controlling blood loss, hemodynamic stability, and surgical field quality. Secondary outcomes were duration of surgery and adverse events. The risk of bias was assessed by the Cochrane Collaboration tool (ROB2). Subgroup and sensitivity analysis was conducted to investigate the study of high risk of bias. Mean difference and relative risk with a 95% confidence interval were used for analysis. There were 15 articles included in the review after screening 615, with a total population of 1143. Clonidine was less blood loss than tranxemic acid (MD=40.17, 95% CI: 4.95- 75.38; p=0.03), more blood loss control than with placebo (MD=-75.15, 95% CI: -96.04-54.25; p <0.00001), and less blood loss control than with dexmedetomidine (MD=7.65, 95% CI: 1.19-14.11; p=0.02). Clonidine maintained mean arterial blood pressure than placebo (MD = -3.87, 95% CI: -6.01--1.72; p = 0.0004). Clonidine is maintained MAP in normal range than placebo when administered Pre-induction (MD=-1.88,95% CI: -3.7--0.07; p=0.04) compared with post induction (MD = -8.16.95% CI: -13.7--2.62; p=0.004). Clonidine has less poor and fair surgical field quality than placebo (RR=0.1, 95% CI: 0.02-0.42, p=0.002; RR=0.82, 95% CI: 0.67-1, p=0.05) respectively. Clonidine decreases blood loss more than placebo. Clonidine is less likely inferior to dexmedetomidine to reducing blood loss for oral and maxillofacial surgery. Clonidine maintains mean arterial blood pressure in the normal range than placebo when administered pre-induction than after induction. Clonidine maintains MAP before induction, and it is effective pre-induction as well as post-induction to maintain a mean heart rate comparable with dexmedetomidine. Clonidine is shortening the duration of surgery comparably with tranxemic acid and dexmedetomidine but more than placebo.},
year = {2026}
}
TY - JOUR T1 - Effectiveness and Safety of Clonidine for Controlling Blood Loss, Hemodynamic Stability, and Surgical Field Quality in Oral and Maxillofacial Surgery: A Systematic Review and Meta-analysis of Randomized Controlled Trials AU - Tesfaye Asefa Hordofa AU - Tajera Tageza Ilala AU - Simon Mengistu Feye AU - Kelil Musa Nerso AU - Dinku Tsegaye Urji AU - Ebrahim Ahmed Hussen Y1 - 2026/04/07 PY - 2026 N1 - https://doi.org/10.11648/j.sdmed.20260102.12 DO - 10.11648/j.sdmed.20260102.12 T2 - Science Discovery Medicine JF - Science Discovery Medicine JO - Science Discovery Medicine SP - 62 EP - 78 PB - Science Publishing Group UR - https://doi.org/10.11648/j.sdmed.20260102.12 AB - Background: Clonidine is an α-adrenoreceptor agonist that reduces sympathetic outflow and releases certain neurotransmitters by acting on receptors in the brain and peripheral tissues. The aim of this systematic review and meta-analysis is about the effectiveness and safety of clonidine for controlling blood loss, hemodynamic stability and surgical field quality comparing with tranxemic acid, placebo and dexmedetomidine. The randomized controlled trials that determine the effect of clonidine on blood loss, hemodynamic stability, and surgical field quality in adult patients undergoing oral and maxillofacial surgery were included. The articles included in this systematic review were searched through the electronic databases PubMed, Cochrane Library, and Google Scholar from July to September 17, 2025. The primary outcomes were controlling blood loss, hemodynamic stability, and surgical field quality. Secondary outcomes were duration of surgery and adverse events. The risk of bias was assessed by the Cochrane Collaboration tool (ROB2). Subgroup and sensitivity analysis was conducted to investigate the study of high risk of bias. Mean difference and relative risk with a 95% confidence interval were used for analysis. There were 15 articles included in the review after screening 615, with a total population of 1143. Clonidine was less blood loss than tranxemic acid (MD=40.17, 95% CI: 4.95- 75.38; p=0.03), more blood loss control than with placebo (MD=-75.15, 95% CI: -96.04-54.25; p <0.00001), and less blood loss control than with dexmedetomidine (MD=7.65, 95% CI: 1.19-14.11; p=0.02). Clonidine maintained mean arterial blood pressure than placebo (MD = -3.87, 95% CI: -6.01--1.72; p = 0.0004). Clonidine is maintained MAP in normal range than placebo when administered Pre-induction (MD=-1.88,95% CI: -3.7--0.07; p=0.04) compared with post induction (MD = -8.16.95% CI: -13.7--2.62; p=0.004). Clonidine has less poor and fair surgical field quality than placebo (RR=0.1, 95% CI: 0.02-0.42, p=0.002; RR=0.82, 95% CI: 0.67-1, p=0.05) respectively. Clonidine decreases blood loss more than placebo. Clonidine is less likely inferior to dexmedetomidine to reducing blood loss for oral and maxillofacial surgery. Clonidine maintains mean arterial blood pressure in the normal range than placebo when administered pre-induction than after induction. Clonidine maintains MAP before induction, and it is effective pre-induction as well as post-induction to maintain a mean heart rate comparable with dexmedetomidine. Clonidine is shortening the duration of surgery comparably with tranxemic acid and dexmedetomidine but more than placebo. VL - 1 IS - 2 ER -
Department of Anesthesia, Madda Walabu University, Robe Bale, Ethiopia
Department of Anesthesia, Hawassa University, Hawassa, Ethiopia
Department of Anesthesia, Madda Walabu University, Robe Bale, Ethiopia
Department of Anesthesia, Madda Walabu University, Robe Bale, Ethiopia
Department of Anesthesia, Madda Walabu University, Robe Bale, Ethiopia
Department of Anesthesia, Madda Walabu University, Robe Bale, Ethiopia
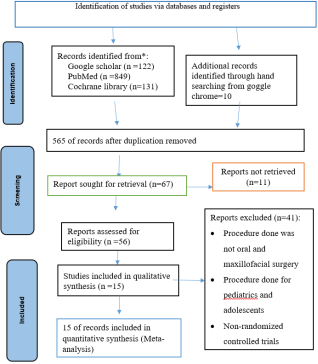
Figure 1. PRISMA Flow chart shows clonidine for controlling of blood loss, hemodynamic stability and surgical field quality among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
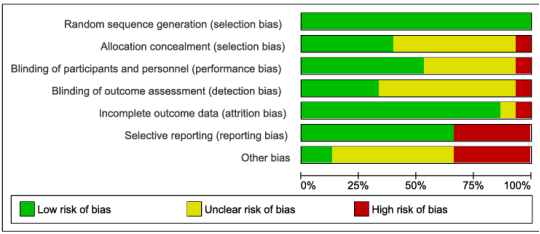
Figure 2. Risk of bias graph of Clonidine for controlling of blood loss, hemodynamic stability and Surgical field quality among adult patient undergoing oral and maxillofacial surgery, SRMA, 2025.
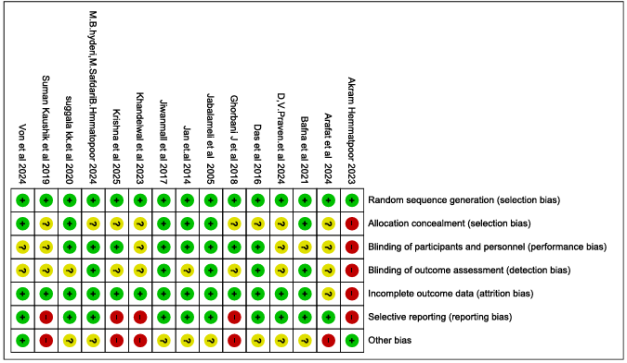
Figure 3. Risk of bias summary of clonidine for controlling of blood loss, hemodynamic stability and surgical field quality among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.

Figure 4. Forest plot shows of comparing clonidine versus tranxemic acid on blood loss controlling among adult patients undergoing oral and maxillofacial surgery, SRMAM, 2025.
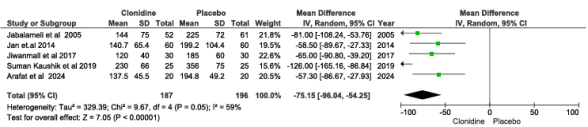
Figure 5. Forest plot shows comparing of clonidine versus placebo on controlling of blood loss among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
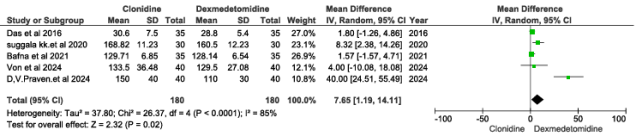
Figure 6. Forest plot shows comparison of clonidine 3.5.2 versus dexmedetomidine on blood loss among adult patients undergoing oral and maxillo-facial surgery, SRMA, 2025.
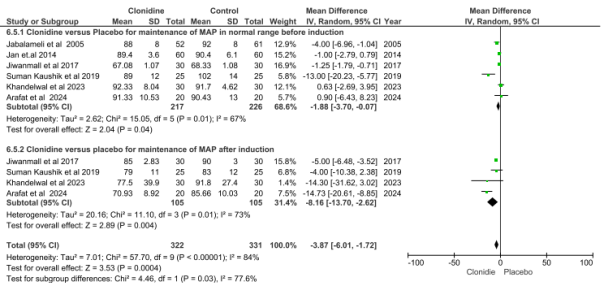
Figure 7. Forest plot shows comparison of clonidine versus placebo on maintenance of Mean arterial pressure among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
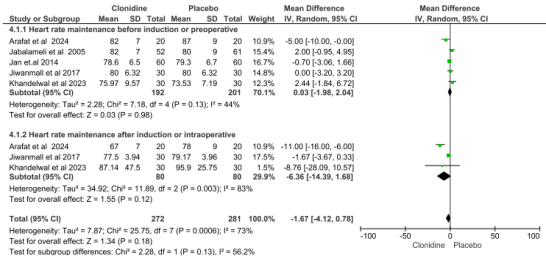
Figure 8. Forest plot shows comparison of clonidine versus placebo on maintenance of mean heart rate among adult patients undergoing oral and maxilla 3 facial surgery, SRMA, 2025.
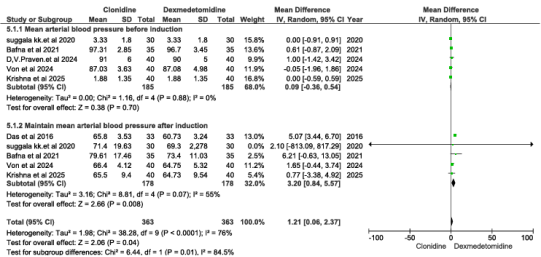
Figure 9. Forest plot shows comparison of clonidine versus dexmedetomidine on maintenance of mean arterial pressure among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
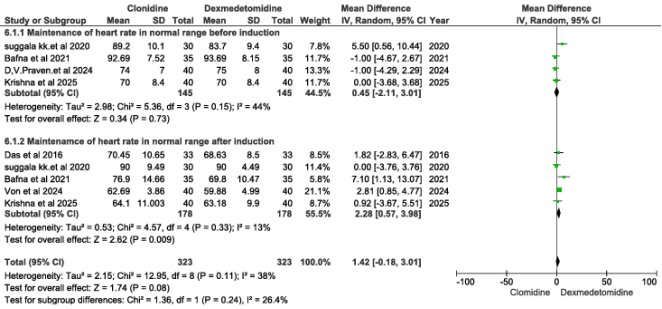
Figure 10. Forest plot shows comparison of clonidine versus dexmedetomidine on maintenance of heart rate among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.

Figure 11. Forest plot comparison of clonidine and TXA on duration of surgery among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.

Figure 12. Forest plot shows comparison of clonidine versus placebo on duration of surgery among adult patients undergoing oral and maxillofacial surgery, 2025.

Figure 13. Forest shows comparison of clonidine versus dexmedetomidine on duration surgery among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
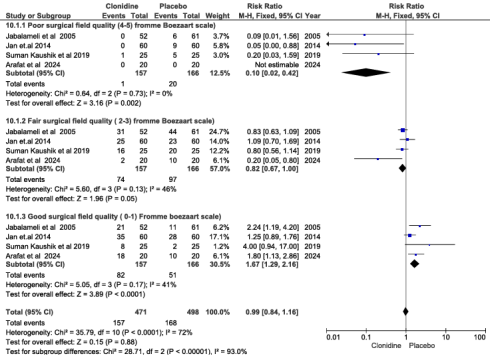
Figure 14. Forest plot shows comparison of clonidine versus placebo on surgical field quality among adult patients undergoing oral and maxillofacial surgery, 2025.
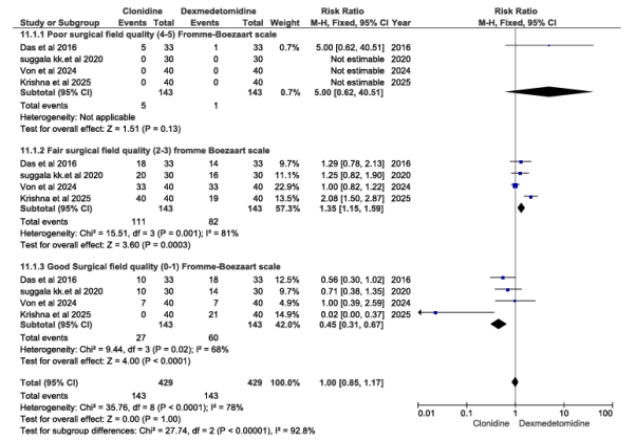
Figure 15. Forest plot shows comparison of clonidine versus dexmedetomidine on surgical field quality among adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
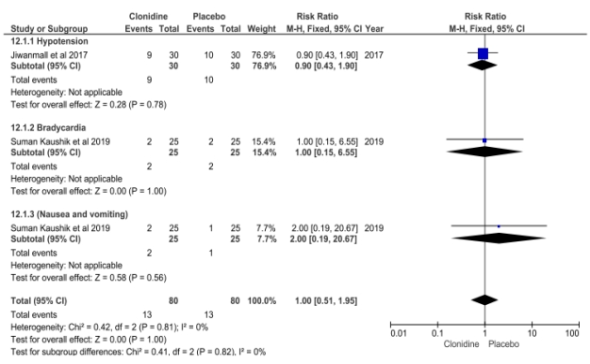
Figure 16. Forest plot shows comparison of clonidine versus placebo on adverse eventamong adult patients undergoing oral and maxillofacial surgery, SRMA, 2025.
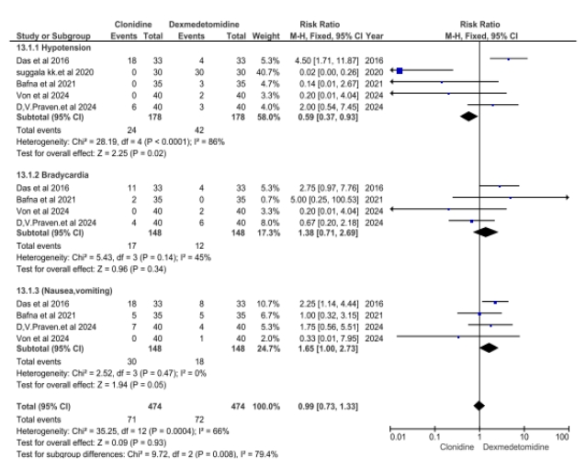
Figure 17. Forest plot shows comparison of clonidine versus dexmedetomidine regarding to adverse reaction among adult patients undergoing oral and maxilla facial surgery, SRMA, 2025.
Information

