Abstract
Severe acute malnutrition (SAM) is the most severe and visible form of undernutrition and remains a major cause of morbidity and mortality in developing countries, particularly in Sub-Saharan Africa. Despite its public health significance, limited studies especially multicenter studies have been conducted in Ethiopia, including the present study area. Therefore, this study aimed to assess the time to achieve target mid-upper arm circumference (MUAC) and its predictors among children with severe acute malnutrition treated in the outpatient therapeutic feeding program (OTP) in Hossana Town, Central Ethiopia. A retrospective follow-up study was conducted among 631 children with SAM enrolled in OTP using systematic random sampling. Kaplan–Meier survival analysis was used to estimate the time to achieve target MUAC, and Cox proportional hazards regression analysis was employed to identify independent predictors. Variables with a p-value <0.25 in the bivariable analysis were included in the multivariable Cox regression model, and statistical significance was declared at p-value <0.05. A total of 631 children were included in the study. The incidence rate of achieving target MUAC was 17.7 per 1000 child-days of observation. Overall, 94.9% of children achieved the target MUAC, while 5.31% were censored (2.16% lost to follow-up and 3.15% referred). The median time to achieve target MUAC was 60 days (IQR: 54–65). Factors significantly associated with time to achieve target MUAC included the presence of cough (AHR = 0.39; 95% CI: 0.30–0.51), inappropriate consumption of ready-to-use therapeutic food (RUTF) (AHR = 0.21; 95% CI: 0.17–0.26), and HIV/AIDS infection (AHR = 0.42; 95% CI: 0.22–0.77). In conclusion, the time to achieve target MUAC was significantly influenced by cough, HIV/AIDS infection, and inappropriate RUTF consumption. Therefore, providing special attention and appropriate management for children with these conditions is essential to improve recovery outcomes and reduce the duration of treatment in OTP programs.
|
Published in
|
Science Discovery Medicine (Volume 1, Issue 1)
|
|
DOI
|
10.11648/j.sdmed.20260101.15
|
|
Page(s)
|
24-37 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Central Ethiopia, Severe Acute Malnutrition, Target MUAC and Under-5 Children
1. Introduction
1.1. Background
Severe acute malnutrition (SAM) is one of the most common causes of morbidity and mortality among children under the age of 5 years worldwide
. Severe acute malnutrition (SAM) refers to all deviations from adequate nutrition that endangers children’s survival, health, growth and development
| [2] | De Onis M, Blössner M. The World Health Organization global database on child growth and malnutrition: methodology and applications. International Journal of Epidemiology. 2003; 32(4): 518–526. https://doi.org/10.1093/ije/dyg099 |
[2]
. Severe acute malnutrition is usually the result of a combination of inadequate dietary intake and infection which is result from multiple causes. Of these, sudden reduction in food intake and reduced quality of diet in combination with a pathological cause is more pronounced
. Acute malnutrition can be categorized into two types: severe acute malnutrition, which is characterized by a weight-for-height z-score <-3 or a mid-upper arm circumference (MUAC) < 11.5 cm and moderate acute malnutrition, which is defined by a z-score between -2 and -3 or a MUAC between 11.5 and 12.5 cm
| [4] | Ariza NR, Nadhiroh SR, Willmart AC. Mid Upper Arm Circumference (MUAC) Accuracy in Detecting Acute Malnutrition in Children under 5 Years: A Literature Review. Amerta Nutrition. 2023, 7(2SP), 328–335.
https://doi.org/10.20473/amnt.v7i2SP.2023.328335 |
[4]
.
“SAM is characterized by the presence of at least one of the following clinical parameters presence of bilateral pitting edema, wasting, Mid-Upper Arm Circumference (MUAC ≤ 11.5), Weight-For-Height (WFH) <-3 z-scores and Weight-For Length (WFL) < -3 z-scores
| [5] | Kliegman RM, Stanton BM, Geme JS. Nelson textbook of pediatrics, 2-volume set, 20th edition. 2015. |
[5]
.”
According to WHO 2021 those children with a MUAC less than 11.5 cm have a highly elevated risk of death compared to those who are counterpart. Thus it is recommended to increase the cut-off point from 110 to 115 mm to define SAM with MUAC
| [6] | World Health Organization, United Nations Children’s Fund (UNICEF), The World Bank Group. Levels and Trends in Child Malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates Key Findings of the 2021 Edition. World Health Organization. 2021. Available from:
https://www.who.int/publications/i/item/9789240025257 |
[6]
.
Severe Acute Malnutrition in childhood has many adverse consequences for child survival and long-term well-being like; cognitive functions, reduces immunity to disease, increases susceptibility to chronic illness, limits livelihoods opportunities and reduces the ability to engage within the community
| [7] | Sphere Association. The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response. 4th ed. Practical Action Publishing; 2018. Available from:
https://spherestandards.org/handbook-2018/ |
| [8] | Baye K, Hirvonen K. Accelerating progress in improving diets and nutrition in Ethiopia. ESSP Research Note 75, International Food Policy Research Institute; 2020.
https://doi.org/10.2499/p15738coll2.133765 |
[7, 8]
.
According to Ethiopian standard set for the management of SAM, children should be recovered from SAM within 56 days of OTP follow up (1). Using a discharge criterion based on percentage MUAC gain has the advantage of being easy to apply to children admitted based on MUAC as well to those admitted on weight-for-height. It is possible to use >12.5cm as discharge criterion for all infants and children admitted to therapeutic feeding programs (6).
The children with SAM are still devastatingly growing globally. It is the third most contributing factor for the death of under-5 children over the entire globe. It is a global public health problem that majorly affects the survival of children 6-59 month of age. Globally, an estimated 555 million children were under five years of age and of these 52 million were suffering from acute malnutrition. More than 90% of those with acute malnutrition live in the developing countries
. As a result it can increase the fatality rate in children suffering from diarrhea and pneumonia in developed and developing countries
| [11] | Joosten KF, Hulst JM. Prevalence of malnutrition in pediatric hospital patients, 2018; 20(5): 590-6.
https://doi.org/10.1097/MOP.0b013e32830c6ede |
| [12] | Bourke CD, Berkley JA, Prendergast AJ. Immune dysfunction as a cause and consequence of malnutrition. Trends in immunology. 2016; 37(6): 386-98. |
[11, 12]
.
Among those children living with severe acute malnutrition; 2 to 3 million die every year and 25 to 30% of the deaths are in poor countries
| [13] | Organization WH. Community-based management of severe acute malnutrition: a joint statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children's Fund: World Health Organization; 2017.
https://www.who.int/publications/i/item/9789241502054 |
[13]
. According to WHO 2021 those children with a MUAC less than 11.5 cm have a highly elevated risk of death compared to those who are counterpart. Thus it is recommended to increase the cut-off point from 110 to 115 mm to define SAM with MUAC
| [6] | World Health Organization, United Nations Children’s Fund (UNICEF), The World Bank Group. Levels and Trends in Child Malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates Key Findings of the 2021 Edition. World Health Organization. 2021. Available from:
https://www.who.int/publications/i/item/9789240025257 |
[6]
.
In Africa, more than 14.0 million under-5 children are wasted, of which 4.1 million children are severely wasted. A cohort study done in Malawi showed a substantial mortality rate 23% of children especially among marasmic children, with a hospital stay ranging from 13 to 33 days
| [14] | Attia S, Versloot CJ, Voskuijl W, van Vliet SJ, Di Giovanni V, Zhang L, et al. Mortality in children with complicated severe acute malnutrition is related to intestinal and systemic inflammation: an observational cohort study. The American journal of clinical nutrition. 2016; 104(5): 1441-9.
https://doi.org/10.3945/ajcn.116.130518 |
[14]
. About 9% of sub-Saharan African and 15% of South Asian children have moderate acute malnutrition and about 2% of children in developing countries have SAM
| [15] | Nalwanga D, Musiime V, Kizito S, Kiggundu JB, Batte A, Musoke P, et al. Mortality among children under five years admitted for routine care of severe acute malnutrition: a prospective cohort study from Kampala, Uganda. BMC pediatrics. 2020; 20(1): 1-11.
https://doi.org/10.1186/s12887-020-02094-w |
[15]
. The burden of malnutrition varies from country to country Yemen is 45.4, Central Africa Republic 45.1%, Democratic Republic of Congo 37.8%, Lesotho 32.4%, and Sierra Leon 3l.5%
.
According to the 2019 Ethiopian Mini Demographic and Health Survey (EDHS) report, 37%, 21% and 7% of children under-5 years of age were stunted, underweight and wasted in Ethiopia respectively. In Southern Ethiopia, 36.3%, 19.7% and 6.3% were stunted, underweight and wasted, respectively
. It has also significantly contributed for impaired intellectual development of children, increased the risk for disease and it is one of the main reasons for children’s hospital admission
| [18] | Girum T, Kote M, Tariku B, Bekele H. Survival status and predictors of mortality among severely acute malnourished children< 5 years of age admitted to stabilization centers in Gedeo Zone: a retrospective cohort study. Therapeutics and clinical risk management. 2017: 101-10.
https://doi.org/10.2147/TCRM.S119826 |
[18]
. The risk of death is 9 times higher for children with SAM than that of children without SAM
| [19] | Teferi E, Lera M, Sita S, Bogale Z, Datiko DG, Yassin MA. Treatment outcome of children with severe acute malnutrition admitted to therapeutic feeding centers in Southern Region of Ethiopia. Ethiopian Journal of Health Development. 2019; 24(3).
https://doi.org/10.4314/ejhd.v24i3.68392 |
[19]
. Each year about 3 million children with SAM are die due to its effect in reducing their immunity against infections as it increases the severity and frequency of the infections and delays to achieve their target MUAC
| [20] | Organization WH. Levels and trends in child malnutrition child malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates: Key findings of the 2023 edition: World Health Organization; 2023.
https://www.who.int/publications/i/item/9789240073791 |
[20]
.
Till recently, the management of SAM has been delivered only at hospitals with limited coverage and accessibility to the problem. However, only 10% of the affected children got treatment from hospital
. About 85% of children with SAM without medical complications were treated at OTP or home
| [22] | Atnafe B, Roba KT, Dingeta T. Time of recovery and associated factors of children with severe acute malnutrition treated at outpatient therapeutic feeding program in Dire Dawa, Eastern Ethiopia. PloS one. 2019; 14(6): e0217344.
https://doi.org/10.1371/journal.pone.0217344 |
[22]
. In response to this there are two major approaches that the government was applied to address malnutrition; first community management of acute malnutrition program was started to make services accessible and available of food through improved economic growth and agricultural production system along with the advancement of good nutrition practices and prevention of malnutrition. Second reinforce early warning systems and timely emergency response including wide-scale delivery of services for the management of acute malnutrition
. On the other hand there is a forgotten issue that focuses on their target Mid-Upper Arm Circumference (MUAC) which is the major indicator of their improvement. So this research aimed to assess the time consumed to achieve the target MUAC.
The OTP is a part of the routine health care services to treat malnutrition that has been provided at both health centers and health posts. The health care services include diagnoses of children with SAM within health facilities, provide ready-to-use therapeutic foods (RUTF), usually Plumpy’ Nut that has been given every week to be eaten at home and a routine medications including amoxicillin, folic acid, measles vaccine, vitamin-A and de-worming. Solely children who don’t have medical complications and have passed the appetite test with Plumpy’Nut are suitable to the OTP
| [24] | Tadesse E, Ekström E-C, Berhane Y. Challenges in implementing the integrated community-based outpatient therapeutic program for severely malnourished children in rural southern Ethiopia. Nutrients. 2016; 8(5): 251.
https://doi.org/10.3390/nu8050251 |
[24]
.
However, the majority of previous studies were conducted in hospitals and health centers on their recovery time without considering their achieving the target MUAC. To the best of our knowledge, there is a lack of evidence on the predictors of time-to-achieve target MUAC among SAM children. The predictors of time to achieve target MUAC in such peripheral institutions would imply an in sight for interventions.
1.2. Significance of the Study
Though Ethiopia has made considerable achievement in the reduction of under-five mortality rate, SAM is still the third most contributing factor for the death of under-5 children. So the trend in reduction is slower
| [25] | Hailegebreal S, Gilano G, Simegn AE, Seboka BTJPo. Spatial variation and determinant of home delivery in Ethiopia: Spatial and mixed effect multilevel analysis based on the Ethiopian mini demographic and health survey 2019. 2022; 17(3): e0264824. https://doi.org/10.1371/journal.pone.0264824 |
[25]
. There is a lack of studies on time to achievement of adequate target among children treated for SAM at outpatient therapeutic feeding program which is important indicator of SAM patient`s improvement.
Hence, the input from this study will provide a base line data:
Understanding how long it takes to achieve a target MUAC provides insight into the effectiveness of different treatment methods and interventions for malnutrition. This information can inform decisions about which approaches are most successful and should be prioritized in future interventions.
Time-to achieve-target-MUAC data can help to predict the expected recovery time for individuals undergoing treatment for malnutrition. This information is valuable for setting realistic expectations for patients and their families, as well as for healthcare providers in planning and resource allocation.
Time-to-achieve target-MUAC data can contribute to research on malnutrition treatment outcomes and program effectiveness. It helps to evaluate the success of interventions at both the individual and population levels, informing future policies and interventions aimed at addressing malnutrition.
Findings from this study will also offer input to decision-makers, program implementers, monitors and evaluators. It also improves health professions’ awareness about predictors of time to achieve target MUAC on SAM children which is important for early re-assessment and take intervention accordingly.
Finally, the results of this study will serve as inputs for further studies.
1.3. Objective of the Study
1.3.1. General Objective
To assess time to achieve target Mid Upper Arm Circumference and its predictors among children with severe acute malnutrition treated at outpatient therapeutic feeding program in Hossana town, central Ethiopia, 2025.
1.3.2. Specific Objective
1) To determine the median time to achieve target Mid Upper Arm Circumference among severe acute malnutrition children treated at outpatient therapeutic feeding program in Hossana Town, Central Ethiopia, Ethiopia, 2025.
2) To identify the predictors that affect time to achieve target Mid Upper Arm Circumference among severe acute malnourished children treated at outpatient therapeutic feeding program in Hossana Town, Central Ethiopia, Ethiopia, 2025.
2. Methods and Materials
2.1. Study Area and Period
This study was carried out from September 15th to October 15th, 2024 among under five children with severe acute malnutrition treated at an outpatient therapeutic feeding program in Hossana Town, Central Ethiopia, Ethiopia, 2025.
Hossana is located in Hadiya zone which is the capital city of Central Ethiopia Regional state and 232 km far from Addis Ababa, Ethiopia. There are four health centers in Hossana town. All four facilities were included in the study. Namely; Heto Health Center (HHC), Mobil Health Center (MHC), Bobicho Health Center (BHC) and Lichamba Health Center (LHC) was included in the study.
2.2. Study Design
Retrospective follow up study was conducted.
2.3. Population
2.3.1. Source Population
Children aged 6-59 months with severe acute malnutrition admitted with MUAC <11.5cm and treated at outpatient therapeutic feeding program.
2.3.2. Study Population
Randomly selected chart of children aged 6-59 months who were enrolled to Outpatient.
Therapeutic feeding program for SAM at health centers Hossana Town from 1st January 2020 to 1st January 2024.
2.4. Eligibility Criteria
Those children admitted with WFH and Bilateral pitting edema with MUAC >11.5cm were excluded.
2.5. Sample Size Determination
The sample size was determined for common predictors that are found to be significantly associated with time-to-achieve target MUAC among SAM Patient admitted under OTP. All the possible sample sizes were calculated, and the largest sample size (
n =631) was selected from the retrospective cohort study conducted in Dire Dawa, Eastern Ethiopia, by considering a major predictor using the Freedman method of sample size determination
| [22] | Atnafe B, Roba KT, Dingeta T. Time of recovery and associated factors of children with severe acute malnutrition treated at outpatient therapeutic feeding program in Dire Dawa, Eastern Ethiopia. PloS one. 2019; 14(6): e0217344.
https://doi.org/10.1371/journal.pone.0217344 |
[22]
. The total sample size was calculated as:
The sample size was determined by using STATA software version 14.0.
The total sample size is calculated by;
Where: n = total sample size needed
E = the number of events that interested
Pr(E) = the probability that the event of interest occurs
Where: E = number of events that interested
Zα/2: Z value at 95% confidence interval = 1.96.
Zβ: the power of the study = 0.8
AHR: Adjusted Hazard Ratio and
IR= incidence rate (17.23%) as obtained from study in Dire Dawa, Eastern Ethiopia on OTP
| [22] | Atnafe B, Roba KT, Dingeta T. Time of recovery and associated factors of children with severe acute malnutrition treated at outpatient therapeutic feeding program in Dire Dawa, Eastern Ethiopia. PloS one. 2019; 14(6): e0217344.
https://doi.org/10.1371/journal.pone.0217344 |
[22]
.
2.6. Sampling Procedure
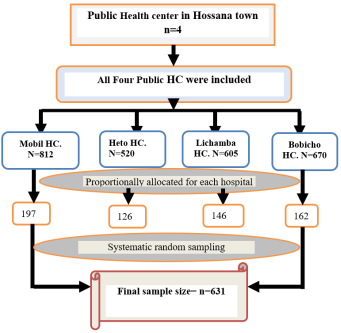
The study included the four public health centers in Hossana Town, Ethiopia. Those are Mobil HC, Bobicho HC, Lichamba HC and Heto HC. For record reviews, four consecutive years (January 1, 2020 to January 1, 2024) were chosen. Starting from the recent month backward, based on the sequence of their card number, a systematic sampling procedure was used to select an adequate number of samples (patient charts).
During a three-year period, there were 2607 admissions of 6-59 month of age children with severe acute malnutrition (SAM). To ensure representative sampling, we were allocated the total sample size proportionally for each health centers: 812 for Mobil HC, 670 for Bobicho HC, 605 for Lichamba HC and 520 for Heto HC. The sampling interval was calculated as k=N/n, where N is 2607 and n is 631, resulting in an interval of 4. Therefore, the data collection was by reviewing every 4
th medical chart consecutively over the three years, starting with a randomly selected chart. This process was consistent for all HCs (
Figure 1).
Figure 1. Schematic representation of sampling procedure for determining time to achieve target MUAC and its predictors among severe acute malnourished children treated at outpatient therapeutic feeding program in Hossana Town, Central Ethiopia, Ethiopia, 2025.
2.7. Variables
2.7.1. Dependent Variable
Time to achieve target Mid Upper Arm Circumference
2.7.2. Independent Variable
Socio Demographic-related factors:-Age of the child, Gender of the child and Place of Residence
Anthropometric related factors:-W/H at admission H/A at admission, Height and Weight.
Treatment & Supplements Related factors:-Deworming, Folic acid, oral antibiotic/s and RUTF use.
Medical complication factors:-Fever, Cough, Diarrhea, Dehydration, Edema, HIV/AIDS, Presence of TB.
Operational definitions
Time to achieve target MUAC:-number of days it takes from admission until a child is achieving discharge criteria for MUAC.
Achieve target MUAC: SAM children that achieve discharge criteria for MUAC is stayed for 8 weeks (56 days) which is stated by Ethiopian standard treatment guideline of SAM
.
Event: refers to achieving the target MUAC during the study period.
Censored: Those children whose death report is recorded, left against medical advice, non-responded to treatment, transferred to in patient therapeutic feeding and lost during treatment with unknown status.
Inappropriate consumption of RUTF: those children who do not come on the date of their appointment.
Severe Acute Malnutrition criteria: children with bilateral pitting edema or severe wasting (MUAC <11.5 cm or WFH-z score<−3), or WFL-z score<−3) and WFA-z score<−3)
| [6] | World Health Organization, United Nations Children’s Fund (UNICEF), The World Bank Group. Levels and Trends in Child Malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates Key Findings of the 2021 Edition. World Health Organization. 2021. Available from:
https://www.who.int/publications/i/item/9789240025257 |
[6]
.
Discharge criteria from OTP: When the child attained WFH>-2 or achieve the target weight or MUAC>12.5cm and no edema for two consecutive visits for edematous SAM.
RUTF consumption appropriate for weight: appropriate amount of RUTF was calculated based on the national SAM management protocol standing from weight of respective children.
Weight gain (g/kg/day): is average weight (in gram) increase for every Kg of body weight of the child per day. And classified as Poor weight gains (< 5 g/kg per day), moderate (5–10 g/kg per day) and good (> 10 g/kg per day)
2.8. Data Collection Tool and Procedure
2.8.1. Data Collection Tool
A structured data abstraction form was used for data collection. The data abstraction form was adopted from another peer-reviewed article conducted in Ethiopia
| [32] | Dagim Biratu SZ, Ebissa Negera, Alemu aS. Achievement of adequate weight gain among infants and children with complicated severe acute malnutrition receiving treatment in therapeutic feeding centers of South Sudanese refugee camps in Ethiopia. 2023. |
[32]
and the sphere standard for management of severe acute malnutrition. The data abstraction contains four parts; like socio-demographic data, medical complication, Anthropometric related factors, Patient’s condition related factors and Treatment & Supplements Related factors which were collect from medical records.
2.8.2. Data Collection Procedure
All available information on patient records was checked in the selected HC in Hossana town, Central Ethiopia, Ethiopia, 2024. From January 1st, 2020 to January 1, 2024 was retrieved from the outpatient Health Management Information System registry book.
The time from the admission was the starting point for retrospective follow-up and the end point was the date of achieving the target MUAC. The date of loss of follow-up or censored (Death, referred or left against medical treatment). All charts admitted to the selected HCs from January 1, 2020 to January 1, 2024 were checked from the registration book.
The records of all study participants were selected according to the eligibility criteria. Achieving the target MUAC was confirmed by observing from SAM chart which was filled by trained nurse. Time of achieving was calculated from the date of admission to the date of achieving the target MUAC.
2.9. Data Quality Control
To ensure the quality of the data, supervisors and data collectors were trained on how and what information they should collect from the targeted data sources. Prior to data collection, the data extraction form was tested on 5% (32 charts) of charts with at Shurmo Health Center before data collection to ensure that the data abstraction format was consistent with study requirements. Completeness of the extracted data was checked on site daily basis during data collection and give prompt feedback by the supervisor and the principal investigator. During data management, storage, cleaning and review, all completed data collection forms were checked for completeness and accuracy.
Two MSc for supervision and four BSc Nurse for data collection were assigned. One day training was given to data collectors and supervisors regarding the significance of the study and ways of data collection process. The supervisors monitor the data collection process. The principal investigator examines consistency by selecting cards at random and comparing their similarity.
2.10. Data Processing and Analysis
Data was cleaned, edited and coded by using Epi data version 3.1. Consistency of data was also checked before analysis to avoid errors during data entry. After that, it was exported to STATA 14 for analysis. The data was checked for missing, fulfillment of assumptions. Graphs, texts and frequency tables were used to report the descriptive data.
Before performing Cox-proportional hazard regression, the model and goodness-of-fit was checked by Cox Snell residuals and assumptions was also check by using Schoenfeld residual test. For each independent predictor bivariate cox proportional Hazard regression was performed. Multicollinearity was checked for estimating the correlation between all pairs of variables by variance inflation factor value ≥ 10
| [34] | Akinwande MO, Dikko HG, Samson A. Variance inflation factor: as a condition for the inclusion of suppressor variable (s) in regression analysis. Open journal of statistics. 2015; 5(07): 754. https://doi.org/10.4236/ojs.2015.57075 |
[34]
. The variables with p-vale <0.25 in bivariate was included in multivariable cox proportional hazard regression. And p-values <0.05 was used to measure the strength of association and identify statistical significant predictors. The outcome was dichotomized into censored “0” or achieves “1”. Kaplan Meier survival curve and log-rank test was used to describe the survival function for each predictor. Results were presented in text, tables, and graphs based on the type of variable.
2.11. Ethical Consideration
Ethical clearance and approval for this study was obtained from the research ethical review committee of College of Medicine and Health Sciences, Debre Brehan University (protocol number IRB-148). Also, a permission letter was obtained from each hospital manager before the full scale data collection. An informed consent was waived by the ethics committee of College of Medicine and Health Sciences, Debre Brehan University because the study was conducted through review of medical charts. Patients’ names were not recorded. All procedures were performed in accordance with the relevant guidelines and regulations.
2.12. Dissemination of the Result
The results will be disseminated to Debre Birhan University Asrat Weldeyes Health Science Campus School of Nursing and Midwifery, department of Pediatrics and Child Health Nursing in partial fulfillment for Masters of Pediatrics and Child Health Nursing.
The findings and recommendations will be distributed to all public health centers, the Central Ethiopia Region Health Bureau and other organizations working on related areas to be used as a baseline for intervention.
3. Result
3.1. Socio-demographic Characteristics of the Study Participants
The median age was 36 months IQR
and standard deviation was 15.4. About 318(50.3%) of the study participants were females; which contribute 303(50.6%) to achieve their target MUAC. Among study participants, 344(54.5%) were urban, which contributes 325(54.3%) to achieve their target MUAC [
Table 1].
Table 1. Socio demographic related factors among children under OTP with SAM at Health center of Hossana Town, Ethiopia, 2025.
| Discharge status |
Achieve target MUAC | Censored |
Sex of the child | Male | 296(49.4%) | 17(53.1%) |
Female | 303(50.6%) | 15(46.9%) |
Place of residence | Urban | 325(54.3%) | 19(3.1%) |
Rural | 274(45.7%) | 13(2.1%) |
Age the child in months | < 24 months | 203(33.9%) | 5(25%) |
> = 24 months | 396(66.1%) | 27(75%) |
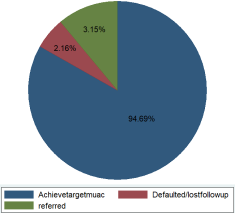
Figure 2. Outcome of severe acute malnutrition children under OTP in Hossana town, Ethiopia, 1st January 2020 to 1st January 2024.
The incidence rate (IR) of achieving target MUAC was 17.7 per 1000 child-days of observation. This indicates that, on average, 9.46 children achieved nutritional recovery per 100 child-days at risk. According to this study about 94.9% were achieve their target MUAC. The children were followed for a total of 35490 day observations [
Figure 2].
3.2. Treatment & Supplements Related Factors
Among the study participants, 312 (49.4%) received deworming medication. Of these, 302 (96.8%) achieved the target MUAC during follow-up. A total of 296 (85.4%) children received folic acid during treatment, with 284 (47.9%) attaining their target MUAC [
Table 2].
Table 2. Treatment & Supplements Related factors among children under OTP with SAM at Health center of Hossana Town, Ethiopia, 2025.
| Discharge status |
Achieve target MUAC | Censored |
Dewormed | Yes | 302(50.4%) | 10(31.2%) |
No | 297(49.6%) | 22(68.8%) |
Child take Folic acid | Yes | 284(47.4%) | 12(37.5%) |
No | 315(52.6%) | 20(62.5%) |
RUTF Consumption | Appropriate consumption | 536(89.5%) | 17(53.1%) |
Inappropriate consumption | 63(9.5%) | 15(46.9%) |
Antibiotic taken | Yes | 107(17.9%) | 13(40.6%) |
No | 492(82.1%) | 19(59.4%) |
3.3. Anthropometric Related Factors
In this study less than half 261 (41.4%) of the participants had 5-10g/kg/day weight gain and 249 (95.4%) of them were achieve their target MUAC. Among 527(83.5%) of children who were admitted with a WFH z-score < −3, 502 (79.5%) were achieved their target MUAC during the study period [
Table 3].
Table 3. Medical complications related factors among children under OTP with SAM at Health center of Hossana Town, Ethiopia, 2025.
| Discharge status |
Achieve target MUAC | Censored |
WFH | WFH z-score < −3 | 476(79.5%) | 22(68.8%) |
WFH z-score ⩾ −3 | 123(20.5%) | 10(31.2%) |
Weight gain/kg/day | Wt gain<5gm/kg/day | 227(37.9%) | 15 (46.5%) |
Wt gain 5-10gm/kg/day | 249(41.7%) | 12(37.5%) |
Wt gain>10gm/kg/day | 128(21.4%) | 5(16.0%) |
WFA | WFA z-score < −3 | 502(83.8%) | 25(78.1%) |
WFA z-score ⩾ −3 | 97(16.2%) | 7(21.9%) |
3.4. Medical Complication Factors
Table 4. Medical complications related factors among children under OTP with SAM at Health center of Hossana Town, Ethiopia, 2025.
| Discharge status |
Achieve target MUAC | Censored |
Presence of edema | Yes | 48(8%) | 4(12.5%) |
No | 551(92.0%) | 28(87.5%) |
Presence of fever | Yes | 15(2.5%) | 4(12.5%) |
No | 584(97.5%) | 28(87.5%) |
Presence of cough | Yes | 72(12.0%) | 9(28.1%) |
No | 527(88.0%) | 23(71.8%) |
Presence of diarrhea | Yes | 27(4.5%) | 2(6.2%) |
No | 572(95.5%) | 30(93.8%) |
Presence of dehydration | Yes | 20(3.3%) | 1(3.1%) |
No | 579(96.7%) | 31(96.9%) |
Presence of HIV/AIDS | Yes | 9(1.5%) | 1(3.1%) |
No | 590(98.5%) | 31(96.9%) |
Presence of TB | Yes | 10(1.7%) | 1(3.1%) |
No | 589(98.3%) | 31(96.9%) |
In the current study 4.6% and 3.3%, children’s had a history of diarrhea and dehydration at admission, respectively. While children who had a history of cough and fever accounts for 12.8% and 3.0% respectively [
Table 4].
Kaplan-Meier Estimates of Time to Achieve Target MUAC among SAM Patients
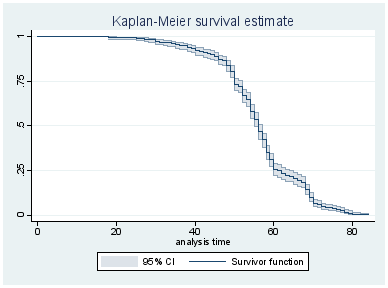
The Kaplan-Meier survival analysis revealed a median time of 60 days (IQR: 54-65) to achieve target MUAC. This estimate represents the time by which 50% of the study population attained nutritional recovery [
Figure 3].
Figure 3. Overall Kaplan-Meier estimates of time to achieve target MUAC among SAM patients who had follow up to health center of Hossana town, Ethiopia, 1st January 2020 to 1st January 2024.
Survival function and comparison for different categorical variables
The Kaplan-Meier estimator was used to analyze and compare the time taken for children with severe acute malnutrition (SAM) to achieve their target mid-upper arm circumference (MUAC) across different categories of weight gain.
The survival curves illustrate the probability of remaining below the target MUAC over time, with lower curves indicating a faster achievement of the target MUAC. Survival function line lying below another means, groups defined by the lower line curve has better to achieve target MUAC than other group line curve within the category.
In this study, children with poor weight gain (<5 g/day) took significantly longer time to reach their target MUAC compared to those with moderate (5–10 g/day) and good weight gain (>10 g/day). The Kaplan-Meier curves demonstrated a clear separation among the three groups, with the poorest weight gain group showing the slowest progression toward target MUAC. The log-rank test confirmed that these differences were statistically significant (p < 0.0001).
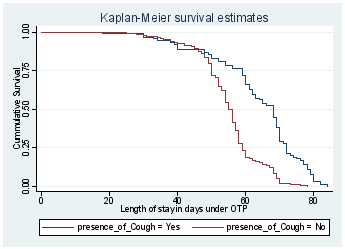
The Kaplan-Meier plot demonstrated a clear divergence between the two groups, with the curve for children with cough lying above that of children without cough, indicating a slower attainment of target MUAC in the former group. This difference was confirmed to be statistically significant (p < 0.0001) by the log-rank test.
These findings suggest that respiratory infections, such as cough, may delay nutritional recovery in children with SAM. This highlights the importance of integrated management of acute malnutrition and respiratory illnesses to improve treatment outcomes and reduce recovery time (
Figure 4).
Figure 4. Hazard function estimates graph for children admitted under OTP in Hossana health centers, from January 2020 to January 2024.
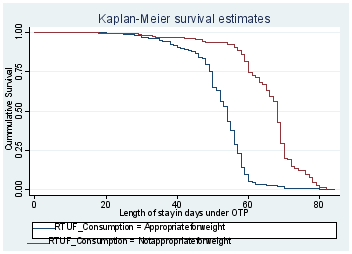
In this study, participants who consumed appropriate RUTF have better time to achieve target MUAC as compared to their counterpart. The difference was statistically significant with a p-value of <0.001 [
Figure 5].
Figure 5. Hazard function estimates graph for children admitted under OTP and their RUTF consumption status in Hossana health centers, from January 2020 to January 2024.
Factor associated with time to achieve target MUAC
The Cox proportional hazard regression model was used to identify determinants of achieving target MUAC of SAM children on follow up. Bivariate analysis was performed first using cox proportional hazard regression to identify which variable had an association with time of achieving their target MUAC.
Those variables like; Presence of cough, RUTF consumption, Presence of edema, Deworming, Presence of diarrhea, Presence of dehydration, Presence of TB and presence of HIV/AIDS were statistically significant with a p-value ≤ 0.25 and candidate for multivariate cox regression.
In a multivariable proportional hazard model; those variables like; RUTF consumption, Presence of cough and presence of HIV/AIDS were the independent predictors of time to achieving target MUAC among SAM children with (p value<0.05).
The multivariable analysis result showed that; the hazard of prolonged time to achieve target MUAC with Cough was 61% delayed than its counterparts. Children with the diagnosis of HIV/AIDS were delayed by 58% in time to achieve target MUAC as compared to children without HIV/AIDS. Similarly, the time to achieve target MUAC with RTUF consumption was prolonged by 79% as compared to its counterparts [
Table 5].
Table 5. Bi-variable and multivariable Cox-proportional hazard analysis of predictors of target MUAC achievement among SAM children under OTP of Hossana health centers, Hossana, CE, Ethiopia, 2024.
Variables | Category | CHR | P-value | AHR | P-vale |
Cough | Yes | 0.36(0.28, 0.46) | <0.001 | 0.39(0.30, 0.51) | <0.001* |
No | 1 | 1 | |
Edema | Yes | 0.78(0.57, 1.07) | 0.103 | 0.96(0.69, 1.33) | 0.808 |
No | 1 | 1 | |
Diarrhea | Yes | 0.79(0.53, 1.17) | 0.002 | 1.18(0.79, 1.76) | 0.405 |
No | 1 | 1 | |
Dehydration | Yes | 0.55(0.36, 0.86) | 0.009 | 0.69(0.44, 1.09) | 0.116 |
No | 1 | 1 | |
HIV/AIDS | Yes | 0.44(0.22, 0.76) | 0.005 | 0.42(0.22, 0.77) | 0.006* |
No | 1 | 1 | |
TB | Yes | 0.43(0.27, 0.69) | 0.001 | 0.84(0.52, 1.37) | 0.502 |
No | 1 | 1 | |
Deworming | Yes | 1.23(1.04, 1.44) | 0.013 | 1.07(0.90, 1.27) | 0.411 |
No | 1 | 1 | |
RUTF consumption | Appropriate | 1 | <0.001 | 1 | |
In appropriate | 0.22(0.18, 0.27) | 0.21(0.17, 0.26) | <0.001* |
Test of proportional-hazards assumption
To use of fitted proportional hazard models, the proportional hazard assumption should be checked. As a result, in this study the Schoenfeld residuals proportional hazard assumption test was used for individual covariates as well as global tests. The proportional hazard assumption is not met if the P-Value is less than 0.05. In this study each covariate has P-Value > 0.05 and all covariates (Global test for Cox proportional hazard P-Value=0.2044 which is also > 0.05 and well met the proportional hazard assumption as shown in [
Table 6].
Table 6. Test of proportional hazard by Schoenfeld residuals for each predictor and global test.
Variables | Rho | Chi2 | Prob>chi2 |
Residence | 0.09574 | 5.55 | 0.0185 |
Sex | 0.01693 | 0.17 | 0.6811 |
Child admission status | 0.03591 | 0.74 | 0.3894 |
Type of SAM | 0.00335 | 0.01 | 0.9187 |
Edema | 0.02151 | 0.45 | 0.9187 |
Fever | -0.00793 | 0.04 | 0.8426 |
Cough | -0.01672 | 0.20 | 0.6582 |
Diarrhea | -0.02874 | 0.51 | 0.4744 |
Dehydration | 0.01603 | 0.16 | 0.6914 |
HIV/AIDS | -0.01506 | 0.13 | 0.7178 |
TB | 0.04070 | 0.96 | 0.3261 |
Deworming | 0.02307 | 0.31 | 0.5782 |
Folic acid | -0.01055 | 0.06 | 0.8028 |
RTUF consumption | 0.09956 | 6.24 | 0.0125 |
Oral antibiotics | 0.05448 | 2.42 | 0.1196 |
Global test | 19.21 | 0.2044 | |
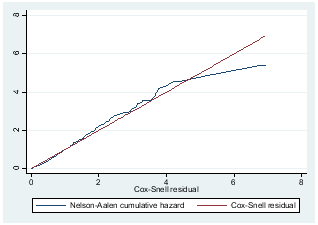
Testing overall fitness of the model
In this study goodness-of-fit was checked graphically using the Cox Snell residuals plot to check the assumption of the Cox proportional hazard model. For the residuals test, the hazard function follows 45° close to the baseline hazard, which indicates that the model was well-fitted. The jagged line with the reference line (Cox Snell residual line) follows the 45° line close.
Figure 6. Cox Snell residual test for proportional assumption of each covariant and overall Cox proportional hazard model.
4. Discussion
This study assessed the time to achieve target Mid Upper Arm Circumference and its predictors among children with severe acute malnutrition treated at outpatient therapeutic feeding program in Hossana town, central Ethiopia. In this study, the children were followed for a total of 35490 day observations.
The result of this study show that, the overall time to achieving target MUAC was 60 days, [IQR; 55, 66]. This result is lower than the study conducted in West Hararghe Zone of Oromia Regional State, Habro Woreda which revealed that; time to cure severe acute malnutrition by MUAC is determined as 10 weeks
| [29] | Lambebo A, DTaTB. Utilization of Mid-Upper Arm Circumference as a Discharge Tool for Children in Outpatient Therapeutic Program, Ethiopia. 2022. Available from: [Journal of Nutritional Science. 2022; 11: e101.]
https://doi.org/10.1017/jns.2022.98 |
[29]
. The observed difference may be due to the variation in sample size difference. And this study was higher than the previous study conducted in south Ethiopia shows that the average length of stay in the program was 35 days for patients with severe wasting and 21 days for patients with edematous malnutrition and 49 in Tigray Ethiopia
| [27] | Kabalo MY, Shanka MM. Seasonal variations of admission and survival status of children treated for severe acute malnutrition (SAM) at outpatient therapeutic program (OTP) in Wolaita Zone, Southern Ethiopia. International Journal of Collaborative Research on Internal Medicine & Public Health. 2016; 8(9): 512-26. |
| [28] | Yebyo HG, Kendall C, Nigusse D, Lemma W. Outpatient therapeutic feeding program outcomes and determinants in treatment of severe acute malnutrition in Tigray, northern Ethiopia: a retrospective cohort study. PloS one. 2013; 8(6): e65840.
https://doi.org/10.1371/journal.pone.0065840 |
[27, 28]
. The observed difference may be due to the above study durations were based on target weight gain from admission but the discharge criteria in this study were on target MUAC or 12.5 cm and discharged from severe acute malnutrition management program by weight gain may not cure of MUAC. This may suggest us children who are declared cured. This may cause their achieving time to be longer than the current study’s median time to achieve the target MUAC. And also higher than the international standard (SPHERE) set for the management of SAM; the median time-to recovery from SAM is 36 days and 56 days Ethiopian standard set for the management of SAM
.
In this study children with cough during their follow up were delayed by 61% in time to achieve the target as compared to their counter parts. This finding is in line with the study done in Amhara region north-west and general hospitals of Tigray region Ethiopia
| [30] | Baraki AG, TYA, Haileab Fekadu Wolde WWT, WNM, Behailu Derseh HDD, Abel Fekadu Dadi. Time to recovery from severe acute malnutrition and its predictors: a multicentre retrospective follow-up study in Amhara region, north-west Ethiopia. 2019. |
| [31] | Gebremicael Guesh GD, Mebrahtu Abay, Berhe Beyene, Ermyas Brhane and Kalayu Brhane. Survival status and predictors of mortality among children with severe acute malnutrition admitted to general hospitals of Tigray, North Ethiopia: a retrospective cohort study. 2018. |
[30, 31]
. The reason may be due to loss of appetite children who had a cough may not eat as much as children who did not. Furthermore infection, metabolic disorder, vomiting and severe dehydration in combination reduce the odds of achieving their target MUAC.
In this study the hazard of prolonged time to achieve target MUAC among SAM patient treated under OTP with HIV/AIDS infection were 58% less likely to achieve their target fast as compared to those children without HIV/AIDS infection. This finding is in line with the study done in Amhara region north-west Ethiopia and general hospitals of Tigray region Ethiopia
| [30] | Baraki AG, TYA, Haileab Fekadu Wolde WWT, WNM, Behailu Derseh HDD, Abel Fekadu Dadi. Time to recovery from severe acute malnutrition and its predictors: a multicentre retrospective follow-up study in Amhara region, north-west Ethiopia. 2019. |
| [31] | Gebremicael Guesh GD, Mebrahtu Abay, Berhe Beyene, Ermyas Brhane and Kalayu Brhane. Survival status and predictors of mortality among children with severe acute malnutrition admitted to general hospitals of Tigray, North Ethiopia: a retrospective cohort study. 2018. |
[30, 31]
. The possible reason could be HIV/AIDS together with malnutrition is particularly fatal because it increases management complexity and opportunistic infection which could impair feeding of SAM children
.
The time to achieve the target MUAC among children with inappropriate RUTF consumption during follow up is delayed by 79% as compared to their counterparts. This finding is in line with the study conducted in Tigray, Bahir Dar and North Shewa Zone of Oromia Region, Ethiopia. This might be due to the reason that, children who received plumpy nut have the possibility to achieve rapid weight gain and reach the discharge criteria earlier than their counterparts
| [36] | Gebremichael DY. Predictors of nutritional recovery time and survival status among children with severe acute malnutrition who have been managed in therapeutic feeding centers, Southern Ethiopia: retrospective cohort study. BMC public health. 2015; 15: 1-11.
https://doi.org/10.1186/s12889-015-1850-7 |
[36]
.
5. Conclusion
In this study, the median time to achieve target MUAC was high as compared to the international standard (SPHERE) set for the management of SAM and Ethiopian standard set for the management of SAM. With regard to determinants; having cough, HIV/AIDS infection, inappropriate RUTF consumption during their follow up period were found statistically significant determinants of time to achieve target MUAC.
6. Recommendation
Based on the findings of this study, the following recommendations have been forwarded with each respective body:
To each health centers
1) Moreover, there were gaps in adherence to SAM management protocol in treating children under OTP at the study area. As this study indicated, insufficient attention to children with lower admission cough, HIV/AIDS infection and low provision of Plumpy Nut affects time of achieving their target MUAC.
2) Provide adequate treatment supplements for better improvement of children.
3) The time to achieve target MUAC is so long and works on shorting of the length of stay under OTP.
To Health professionals
Health care providers should give a special focus to children who have cough, HIV/AIDS infection and inappropriate RUTF consumption during their follow up under OTP. At the site of OTP, give deep nutritional counseling for families that Plumpy Nut is not meant to be a substitute for food and should not be given for healthy children found at home. Provide nutrition education at community level through health extension workers to prevent child under-nutrition and miss use of Plumpy Nut. All concerned bodies should give emphasis on RUTF supply in the region as well as at national level to avoid partial provision of RUTF.
To Future researchers
Better to conduct using prospective cohort study that includes other variables such as parental, socio-demographic and economic characteristics.
Strengths
The study area covers all the health centers in Hossana town and the results in findings can be generalized.
Large sample size was used comparing to the other study done in Ethiopia which increases generalization to population.
Limitations
Since the study was retrospective and centered on secondary data, it did not take into account all possible determinants of the outcome variable, such as parental socio-demographic, socioeconomic and environmental factors.
Abbreviations
HC | Health Center |
MUAC | Mid-Upper Arm Circumference |
OTP | Outpatient Therapeutic Feeding Program |
SAM | Severe Acute Malnutrition |
UNICEF | United Nations Children’s Fund |
WFH | Weight-for-Height |
WFL | Weight-for Length |
WFA | Weight-for Age |
Acknowledgments
We would like to thank Debre Brehan University, Department of Nursing and Midwifery, Hospitals Manager, data collectors and supervisors for their respective support.
Author Contributions
Elias Geneti: Conceptualization, Methodology, Writing – original draft, Writing – review & editing
Wondimu Laemebo: Conceptualization, Writing – original draft
Tesfu Zewdu: Conceptualization, Methodology, Writing – review & editing
Sisay Shewasinad: Methodology, Writing – original draft, Writing – review & editing
Hilina Ketema: Methodology, Writing – review & editing
Data Availability Statement
All data generated or analyzed during this study are included in this article.
Conflicts of Interest
All authors declare no competing interests.
References
| [1] |
Federal Ministry of Health (FMOH). Guidelines for the Management of Common Illnesses in Hospitals. 2nd edition. Adis-Ababa, Ethiopia: FMOH; 2016. Available from:
https://hakimethi.org/wp–content/uploads/2024/09/Pediatric-illness-Tx-guideline-2016.pdf
|
| [2] |
De Onis M, Blössner M. The World Health Organization global database on child growth and malnutrition: methodology and applications. International Journal of Epidemiology. 2003; 32(4): 518–526.
https://doi.org/10.1093/ije/dyg099
|
| [3] |
United Nations Children’s Fund (UNICEF). Nutrition in Emergencies: Saving Lives Today, Strengthening Systems for Tomorrow. 2018. Available from:
https://www.unicef.org/reports/nutrition-in-emergencies-saving-lives-today-strengthening-systems-for-tomorrow
|
| [4] |
Ariza NR, Nadhiroh SR, Willmart AC. Mid Upper Arm Circumference (MUAC) Accuracy in Detecting Acute Malnutrition in Children under 5 Years: A Literature Review. Amerta Nutrition. 2023, 7(2SP), 328–335.
https://doi.org/10.20473/amnt.v7i2SP.2023.328335
|
| [5] |
Kliegman RM, Stanton BM, Geme JS. Nelson textbook of pediatrics, 2-volume set, 20th edition. 2015.
|
| [6] |
World Health Organization, United Nations Children’s Fund (UNICEF), The World Bank Group. Levels and Trends in Child Malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates Key Findings of the 2021 Edition. World Health Organization. 2021. Available from:
https://www.who.int/publications/i/item/9789240025257
|
| [7] |
Sphere Association. The Sphere Handbook: Humanitarian Charter and Minimum Standards in Humanitarian Response. 4th ed. Practical Action Publishing; 2018. Available from:
https://spherestandards.org/handbook-2018/
|
| [8] |
Baye K, Hirvonen K. Accelerating progress in improving diets and nutrition in Ethiopia. ESSP Research Note 75, International Food Policy Research Institute; 2020.
https://doi.org/10.2499/p15738coll2.133765
|
| [9] |
National Guideline for the Management of Acute Malnutrition in Ethiopia. Federal Ministry of Health–Ethiopia; 2021. Available from:
https://msn.moh.gov.et/pdf/moh/Nutrition_Guidelines/FINAL_Ethiopia_Guidelines_for_AM_%20August_21.pdf
|
| [10] |
UNICEF W, World Bank Group. Levels and trends in child malnutrition. UNICEF, World Health Organization, World Bank Group; 2017:
https://www.who.int/publications/m/item/jme–estimates-2017-edition
|
| [11] |
Joosten KF, Hulst JM. Prevalence of malnutrition in pediatric hospital patients, 2018; 20(5): 590-6.
https://doi.org/10.1097/MOP.0b013e32830c6ede
|
| [12] |
Bourke CD, Berkley JA, Prendergast AJ. Immune dysfunction as a cause and consequence of malnutrition. Trends in immunology. 2016; 37(6): 386-98.
|
| [13] |
Organization WH. Community-based management of severe acute malnutrition: a joint statement by the World Health Organization, the World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children's Fund: World Health Organization; 2017.
https://www.who.int/publications/i/item/9789241502054
|
| [14] |
Attia S, Versloot CJ, Voskuijl W, van Vliet SJ, Di Giovanni V, Zhang L, et al. Mortality in children with complicated severe acute malnutrition is related to intestinal and systemic inflammation: an observational cohort study. The American journal of clinical nutrition. 2016; 104(5): 1441-9.
https://doi.org/10.3945/ajcn.116.130518
|
| [15] |
Nalwanga D, Musiime V, Kizito S, Kiggundu JB, Batte A, Musoke P, et al. Mortality among children under five years admitted for routine care of severe acute malnutrition: a prospective cohort study from Kampala, Uganda. BMC pediatrics. 2020; 20(1): 1-11.
https://doi.org/10.1186/s12887-020-02094-w
|
| [16] |
Chakraborty A, Mukhopadhyay S. Global Hunger Index: Misplaced Debate and Ignoring Priorities. URL:
https://www.theindiaforum.in/economy/global-hunger-index-misplaced-debate-and-ignoring-priorities
|
| [17] |
Ephi I. Ethiopian public health Institute (EPHI)[Ethiopia] and ICF. Ethiopia mini demographic and health survey. 2019.
https://dhsprogram.com/pubs/pdf/FR363/FR363.pdf
|
| [18] |
Girum T, Kote M, Tariku B, Bekele H. Survival status and predictors of mortality among severely acute malnourished children< 5 years of age admitted to stabilization centers in Gedeo Zone: a retrospective cohort study. Therapeutics and clinical risk management. 2017: 101-10.
https://doi.org/10.2147/TCRM.S119826
|
| [19] |
Teferi E, Lera M, Sita S, Bogale Z, Datiko DG, Yassin MA. Treatment outcome of children with severe acute malnutrition admitted to therapeutic feeding centers in Southern Region of Ethiopia. Ethiopian Journal of Health Development. 2019; 24(3).
https://doi.org/10.4314/ejhd.v24i3.68392
|
| [20] |
Organization WH. Levels and trends in child malnutrition child malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates: Key findings of the 2023 edition: World Health Organization; 2023.
https://www.who.int/publications/i/item/9789240073791
|
| [21] |
Collins S, Sadler K. Outpatient care for severely malnourished children in emergency relief programmes: a retrospective cohort study. The Lancet. 2018; 360(9348): 1824-30.
https://doi.org/10.1016/S0140-6736(02)11732-6
|
| [22] |
Atnafe B, Roba KT, Dingeta T. Time of recovery and associated factors of children with severe acute malnutrition treated at outpatient therapeutic feeding program in Dire Dawa, Eastern Ethiopia. PloS one. 2019; 14(6): e0217344.
https://doi.org/10.1371/journal.pone.0217344
|
| [23] |
UNICEF WHO, World Bank Group Joint Child Malnutrition Estimates. GLOBAL ACTION PLAN ON CHILD WASTING A framework for action to accelerate progress in preventing and managing child wasting and. 2019.
https://www.who.int/publications/i/item/9789240000178
|
| [24] |
Tadesse E, Ekström E-C, Berhane Y. Challenges in implementing the integrated community-based outpatient therapeutic program for severely malnourished children in rural southern Ethiopia. Nutrients. 2016; 8(5): 251.
https://doi.org/10.3390/nu8050251
|
| [25] |
Hailegebreal S, Gilano G, Simegn AE, Seboka BTJPo. Spatial variation and determinant of home delivery in Ethiopia: Spatial and mixed effect multilevel analysis based on the Ethiopian mini demographic and health survey 2019. 2022; 17(3): e0264824.
https://doi.org/10.1371/journal.pone.0264824
|
| [26] |
Sphere Association. Humanitarian Charter and Minimum Standards in Humanitarian Response. Sphere Handbook. 2018. Available from: URL:
https://www.spherehandbook.org/handbook/
|
| [27] |
Kabalo MY, Shanka MM. Seasonal variations of admission and survival status of children treated for severe acute malnutrition (SAM) at outpatient therapeutic program (OTP) in Wolaita Zone, Southern Ethiopia. International Journal of Collaborative Research on Internal Medicine & Public Health. 2016; 8(9): 512-26.
|
| [28] |
Yebyo HG, Kendall C, Nigusse D, Lemma W. Outpatient therapeutic feeding program outcomes and determinants in treatment of severe acute malnutrition in Tigray, northern Ethiopia: a retrospective cohort study. PloS one. 2013; 8(6): e65840.
https://doi.org/10.1371/journal.pone.0065840
|
| [29] |
Lambebo A, DTaTB. Utilization of Mid-Upper Arm Circumference as a Discharge Tool for Children in Outpatient Therapeutic Program, Ethiopia. 2022. Available from: [Journal of Nutritional Science. 2022; 11: e101.]
https://doi.org/10.1017/jns.2022.98
|
| [30] |
Baraki AG, TYA, Haileab Fekadu Wolde WWT, WNM, Behailu Derseh HDD, Abel Fekadu Dadi. Time to recovery from severe acute malnutrition and its predictors: a multicentre retrospective follow-up study in Amhara region, north-west Ethiopia. 2019.
|
| [31] |
Gebremicael Guesh GD, Mebrahtu Abay, Berhe Beyene, Ermyas Brhane and Kalayu Brhane. Survival status and predictors of mortality among children with severe acute malnutrition admitted to general hospitals of Tigray, North Ethiopia: a retrospective cohort study. 2018.
|
| [32] |
Dagim Biratu SZ, Ebissa Negera, Alemu aS. Achievement of adequate weight gain among infants and children with complicated severe acute malnutrition receiving treatment in therapeutic feeding centers of South Sudanese refugee camps in Ethiopia. 2023.
|
| [33] |
WHO. POCKET BOOK OF Hospital care for children. 2013 2nd EDITION; 2nd; URL:
https://www.who.int/publications/i/item/9789241548373
|
| [34] |
Akinwande MO, Dikko HG, Samson A. Variance inflation factor: as a condition for the inclusion of suppressor variable (s) in regression analysis. Open journal of statistics. 2015; 5(07): 754.
https://doi.org/10.4236/ojs.2015.57075
|
| [35] |
UNICEF. The state of the world’s children 2019: children, food and nutrition: growing well in a changing world: Unicef; 2019.
https://www.unicef.org/reports/state-of-worlds-children-2019
|
| [36] |
Gebremichael DY. Predictors of nutritional recovery time and survival status among children with severe acute malnutrition who have been managed in therapeutic feeding centers, Southern Ethiopia: retrospective cohort study. BMC public health. 2015; 15: 1-11.
https://doi.org/10.1186/s12889-015-1850-7
|
Cite This Article
-
APA Style
Geneti, E., Laemebo, W., Zewdu, T., Shewasinad, S., Ketema, H. (2026). Time to Achieve Target MUAC and Its Predictors Among Children with Severe Acute Malnutrition Under Outpatient Therapeutic Programs, Hossana, Ethiopia. Science Discovery Medicine, 1(1), 24-37. https://doi.org/10.11648/j.sdmed.20260101.15
 Copy
|
Copy
|
 Download
Download
ACS Style
Geneti, E.; Laemebo, W.; Zewdu, T.; Shewasinad, S.; Ketema, H. Time to Achieve Target MUAC and Its Predictors Among Children with Severe Acute Malnutrition Under Outpatient Therapeutic Programs, Hossana, Ethiopia. Sci. Discov. Med. 2026, 1(1), 24-37. doi: 10.11648/j.sdmed.20260101.15
Copy
|
Download
AMA Style
Geneti E, Laemebo W, Zewdu T, Shewasinad S, Ketema H. Time to Achieve Target MUAC and Its Predictors Among Children with Severe Acute Malnutrition Under Outpatient Therapeutic Programs, Hossana, Ethiopia. Sci Discov Med. 2026;1(1):24-37. doi: 10.11648/j.sdmed.20260101.15
Copy
|
Download
-
@article{10.11648/j.sdmed.20260101.15,
author = {Elias Geneti and Wondimu Laemebo and Tesfu Zewdu and Sisay Shewasinad and Hilina Ketema},
title = {Time to Achieve Target MUAC and Its Predictors Among Children with Severe Acute Malnutrition Under Outpatient Therapeutic Programs, Hossana, Ethiopia},
journal = {Science Discovery Medicine},
volume = {1},
number = {1},
pages = {24-37},
doi = {10.11648/j.sdmed.20260101.15},
url = {https://doi.org/10.11648/j.sdmed.20260101.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sdmed.20260101.15},
abstract = {Severe acute malnutrition (SAM) is the most severe and visible form of undernutrition and remains a major cause of morbidity and mortality in developing countries, particularly in Sub-Saharan Africa. Despite its public health significance, limited studies especially multicenter studies have been conducted in Ethiopia, including the present study area. Therefore, this study aimed to assess the time to achieve target mid-upper arm circumference (MUAC) and its predictors among children with severe acute malnutrition treated in the outpatient therapeutic feeding program (OTP) in Hossana Town, Central Ethiopia. A retrospective follow-up study was conducted among 631 children with SAM enrolled in OTP using systematic random sampling. Kaplan–Meier survival analysis was used to estimate the time to achieve target MUAC, and Cox proportional hazards regression analysis was employed to identify independent predictors. Variables with a p-value <0.25 in the bivariable analysis were included in the multivariable Cox regression model, and statistical significance was declared at p-value <0.05. A total of 631 children were included in the study. The incidence rate of achieving target MUAC was 17.7 per 1000 child-days of observation. Overall, 94.9% of children achieved the target MUAC, while 5.31% were censored (2.16% lost to follow-up and 3.15% referred). The median time to achieve target MUAC was 60 days (IQR: 54–65). Factors significantly associated with time to achieve target MUAC included the presence of cough (AHR = 0.39; 95% CI: 0.30–0.51), inappropriate consumption of ready-to-use therapeutic food (RUTF) (AHR = 0.21; 95% CI: 0.17–0.26), and HIV/AIDS infection (AHR = 0.42; 95% CI: 0.22–0.77). In conclusion, the time to achieve target MUAC was significantly influenced by cough, HIV/AIDS infection, and inappropriate RUTF consumption. Therefore, providing special attention and appropriate management for children with these conditions is essential to improve recovery outcomes and reduce the duration of treatment in OTP programs.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Time to Achieve Target MUAC and Its Predictors Among Children with Severe Acute Malnutrition Under Outpatient Therapeutic Programs, Hossana, Ethiopia
AU - Elias Geneti
AU - Wondimu Laemebo
AU - Tesfu Zewdu
AU - Sisay Shewasinad
AU - Hilina Ketema
Y1 - 2026/03/19
PY - 2026
N1 - https://doi.org/10.11648/j.sdmed.20260101.15
DO - 10.11648/j.sdmed.20260101.15
T2 - Science Discovery Medicine
JF - Science Discovery Medicine
JO - Science Discovery Medicine
SP - 24
EP - 37
PB - Science Publishing Group
UR - https://doi.org/10.11648/j.sdmed.20260101.15
AB - Severe acute malnutrition (SAM) is the most severe and visible form of undernutrition and remains a major cause of morbidity and mortality in developing countries, particularly in Sub-Saharan Africa. Despite its public health significance, limited studies especially multicenter studies have been conducted in Ethiopia, including the present study area. Therefore, this study aimed to assess the time to achieve target mid-upper arm circumference (MUAC) and its predictors among children with severe acute malnutrition treated in the outpatient therapeutic feeding program (OTP) in Hossana Town, Central Ethiopia. A retrospective follow-up study was conducted among 631 children with SAM enrolled in OTP using systematic random sampling. Kaplan–Meier survival analysis was used to estimate the time to achieve target MUAC, and Cox proportional hazards regression analysis was employed to identify independent predictors. Variables with a p-value <0.25 in the bivariable analysis were included in the multivariable Cox regression model, and statistical significance was declared at p-value <0.05. A total of 631 children were included in the study. The incidence rate of achieving target MUAC was 17.7 per 1000 child-days of observation. Overall, 94.9% of children achieved the target MUAC, while 5.31% were censored (2.16% lost to follow-up and 3.15% referred). The median time to achieve target MUAC was 60 days (IQR: 54–65). Factors significantly associated with time to achieve target MUAC included the presence of cough (AHR = 0.39; 95% CI: 0.30–0.51), inappropriate consumption of ready-to-use therapeutic food (RUTF) (AHR = 0.21; 95% CI: 0.17–0.26), and HIV/AIDS infection (AHR = 0.42; 95% CI: 0.22–0.77). In conclusion, the time to achieve target MUAC was significantly influenced by cough, HIV/AIDS infection, and inappropriate RUTF consumption. Therefore, providing special attention and appropriate management for children with these conditions is essential to improve recovery outcomes and reduce the duration of treatment in OTP programs.
VL - 1
IS - 1
ER -
Copy
|
Download