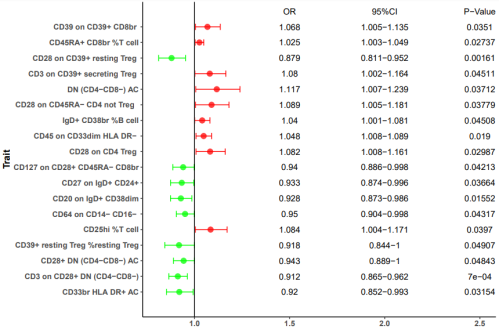
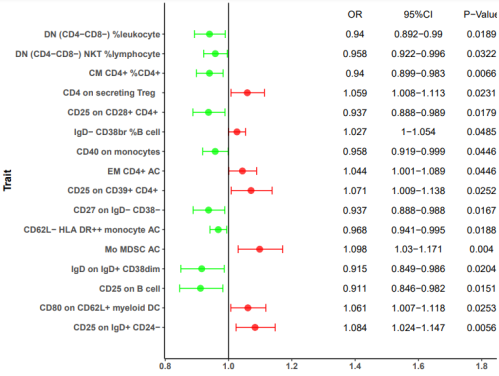
The present Mendelian randomization study investigated the potential causal relationship between immunophenotypes and inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC). Results demonstrated that immunophenotypes, such as CD28 on CD39+ resting Treg and CD25 on IgD+ CD24− showed nominal significant protective effects on CD and UC, respectively. Conversely, specific immunophenotypes also exhibited nominal significant risk effects on CD and UC, including CD39 on CD39+ CD8br and IgD on IgD+ CD38dim, respectively. Collectively, our findings highlight the potential role of immune cell phenotypes in the development of CD and UC as evidenced by data analysis from the FinnGen database. Therefore, the present study contributes to understanding the genetic basis of IBD and highlights the significance of immune cell phenotypes in disease pathogenesis.
| Published in | International Journal of Gastroenterology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijg.20250901.14 |
| Page(s) | 25-31 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Inflammatory Bowel Diseases, Crohn’s Disease, Ulcerative Colitis, Immunity, MR Analysis
IBD | Inflammatory Bowel Diseases |
CD | Crohn’s Disease |
UC | Ulcerative Colitis |
MR | Mendelian Randomization |
MFI | Median Fluorescence Intensities |
IVW | Inverse Variance Weighted |
OR | Odds Ratio |
| [1] | R. Caruso, B. C. Lo, G. Núñez, Host-microbiota interactions in inflammatory bowel disease. Nat Rev Immunol. 20 411-426, |
| [2] | The global, regional, and national burden of inflammatory bowel disease in 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 5 17-30, |
| [3] | M. Agrawal, K. H. Allin, F. Petralia, J. F. Colombel, T. Jess, Multiomics to elucidate inflammatory bowel disease risk factors and pathways. Nat Rev Gastroenterol Hepatol. 19 399-409, |
| [4] | L. Xu, B. He, J. Li, P. Shen, L. Hu, G. Liu, J. Wang, L. Duan, S. Zhan, S. Wang, Incidence of Inflammatory Bowel Disease in Urban China: A Nationwide Population-based Study. Clin Gastroenterol Hepatol. 21 3379-3386.e3329, |
| [5] | G. G. Kaplan, The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 12 720-727, |
| [6] | T. H. Bisgaard, K. H. Allin, L. Keefer, A. N. Ananthakrishnan, T. Jess, Depression and anxiety in inflammatory bowel disease: epidemiology, mechanisms and treatment. Nat Rev Gastroenterol Hepatol. 19 717-726, |
| [7] | M. Agrawal, E. A. Spencer, J. F. Colombel, R. C. Ungaro, Approach to the Management of Recently Diagnosed Inflammatory Bowel Disease Patients: A User's Guide for Adult and Pediatric Gastroenterologists. Gastroenterology. 161 47-65, |
| [8] | A. Sharma, S. Szymczak, M. Rühlemann, S. F. -Wolf, C. Knecht, J. Enderle, S. Schreiber, A. Franke, W. Lieb, M. Krawczak, A. Dempfle, Linkage analysis identifies novel genetic modifiers of microbiome traits in families with inflammatory bowel disease. Gut Microbes. 14 2024415, |
| [9] | Q. Lu, M. -F. Yang, Y. J. Liang, J. Xu, H. -M. Xu, Y. -Q. Nie, L. -S. Wang, J. Yao, D. -F. Li, Immunology of Inflammatory Bowel Disease: Molecular Mechanisms and Therapeutics. J Inflamm Res. 15 1825-1844, |
| [10] | E. Birney, Mendelian Randomization. Cold Spring Harb Perspect Med. 12 |
| [11] | G. S. Davey, G. Hemani, Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Hum Mol Genet. 23 R89-98, |
| [12] | G. Hemani, J. Zheng, B. Elsworth, K. H. Wade, V. Haberland, D. Baird, C. Laurin,. The MR-Base platform supports systematic causal inference across the human phenome. eLife. 7 |
| [13] | V. Orrù, M. Steri, C. Sidore, M. Marongiu, V. Serra, S. Olla, G. Sole, S. Lai, M. Dei, Complex genetic signatures in immune cells underlie autoimmunity and inform therapy. Nat Genet. 52 1036-1045, |
| [14] |
C. Sidore, F. Busonero, A. Maschio, E. Porcu, S. Naitza, M. Zoledziewska, A. Mulas, Genome sequencing elucidates Sardinian genetic architecture and augments association analyses for lipid and blood inflammatory markers. Nat Genet. 47 1272-1281,
https://doi.org/10.1038/ng.3368 (2015). |
| [15] | A. Auton, A. Auton, L. D. Brooks, R. M. Durbin, E. P. Garrison, H. M. Kang, J. O. Korbel,. A global reference for human genetic variation. Nature. 526 68-74, |
| [16] | C. Wang, D. Zhu, D. Zhang, X. Zuo, L. Yao, T. Liu, X. Ge, C. He, Y. Zhou, Z. Shen, Causal role of immune cells in schizophrenia: Mendelian randomization (MR) study. BMC psychiatry. 23 590, |
| [17] | A. J. Noyce, D. A. Kia, G. Hemani, A. Nicolas, T. R. Price, Estimating the causal influence of body mass index on risk of Parkinson disease: A Mendelian randomisation study. PLoS Med. 14 e1002314, |
| [18] | S. Burgess, S. G Thompson, Avoiding bias from weak instruments in Mendelian randomization studies. Int J Epidemiol. 40 755-764, |
| [19] | N. Dimou, K. K. Tsilidis, B. Banbury, R. M. Martin, S. J. Lewis, N. Kazmi, T. M. Robinson, D. Albanes, Physical activity and risks of breast and colorectal cancer: a Mendelian randomisation analysis. Nat Commun. 11 597 |
| [20] | S. Burgess, S. G. Thompson, Interpreting findings from Mendelian randomization using the MR-Egger method. Eur J Epidemiol. 32 377-389, |
| [21] | M. Y. Choy, J. A. Walker-Smith, C. B. Williams, T. T. MacDonald, Differential expression of CD25 (interleukin-2 receptor) on lamina propria T cells and macrophages in the intestinal lesions in Crohn's disease and ulcerative colitis. Gut. 31 1365-1370, |
| [22] | Zheng, Y. W. Ge, Y. Ma, G. Xie, W. Wang, L. Han, B. Bian, L. Li, L. Shen, miR-155 Regulates IL-10-Producing CD24(hi)CD27(+) B Cells and Impairs Their Function in Patients with Crohn's Disease. Front Immunol. 8 914, |
| [23] | N. Oshitani, F. Hato, S. Kitagawa, J. Masuyama, K. Higuchi, T. Matsumoto, T. Arakawal. Expression of 4C8 antigen, a novel transendothelial migration-associated molecule on activated T lymphocytes, in inflammatory bowel disease. Journal Pathol. 197 589-594, |
| [24] | L. Linton, M. Karlsson, J. Grundström, E. Hjalmarsson, A. Lindberg, HLA-DR(hi) and CCR9 Define a Pro-Inflammatory Monocyte Subset in IBD. Clin Transl Gastroenterol. 3 e29, |
| [25] | Mitsialis, V. S. Wall, P. Liu, J. Ordovas-Montanes, T. Parmet,. Single-Cell Analyses of Colon and Blood Reveal Distinct Immune Cell Signatures of Ulcerative Colitis and Crohn's Disease. Gastroenterology. 159 591-608.e510, |
| [26] | X. Wang, Y. Zhu, M. Zhang, H. Wang, Y. Jiang, P. Gao. Ulcerative Colitis Is Characterized by a Decrease in Regulatory B Cells. J Crohns Colitis. 10, 1212-1223, |
| [27] | L. Chapuy, M. Bsat, M. Rubio, S. Sarkizova, A. Therrien, A. Weber, G. Soucy, A. -C. Villani, M. Sarfati, IL-12 and Mucosal CD14+ Monocyte-Like Cells Induce IL-8 in Colonic Memory CD4+ T Cells of Patients With Ulcerative Colitis but not Crohn's Disease. J Crohns Colitis. 14 79-95, |
| [28] | Y. Wang, H. Zhang, H. He, K. Ai, W. Yu, X. Xiao, Y. Qin, L. Zhang, H. Xiong, G. Zhou, LRCH1 suppresses migration of CD4(+) T cells and refers to disease activity in ulcerative colitis. Int J Medical Sci. 17 599-608, |
| [29] | Q. Fan, M. Li, W. Zhao, K. Zhang, M. Li, W. Li. Hyper α2,6-Sialylation Promotes CD4(+) T-Cell Activation and Induces the Occurrence of Ulcerative Colitis. Adv Sci (Weinheim). 10 |
APA Style
Shi, H., Peng, Q. (2025). Causal Role of Immune Cells in Inflammatory Bowel Disease: A Mendelian Randomization (MR) Study. International Journal of Gastroenterology, 9(1), 25-31. https://doi.org/10.11648/j.ijg.20250901.14
ACS Style
Shi, H.; Peng, Q. Causal Role of Immune Cells in Inflammatory Bowel Disease: A Mendelian Randomization (MR) Study. Int. J. Gastroenterol. 2025, 9(1), 25-31. doi: 10.11648/j.ijg.20250901.14
@article{10.11648/j.ijg.20250901.14,
author = {Heng Shi and Qin Peng},
title = {Causal Role of Immune Cells in Inflammatory Bowel Disease: A Mendelian Randomization (MR) Study
},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {1},
pages = {25-31},
doi = {10.11648/j.ijg.20250901.14},
url = {https://doi.org/10.11648/j.ijg.20250901.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250901.14},
abstract = {The present Mendelian randomization study investigated the potential causal relationship between immunophenotypes and inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC). Results demonstrated that immunophenotypes, such as CD28 on CD39+ resting Treg and CD25 on IgD+ CD24− showed nominal significant protective effects on CD and UC, respectively. Conversely, specific immunophenotypes also exhibited nominal significant risk effects on CD and UC, including CD39 on CD39+ CD8br and IgD on IgD+ CD38dim, respectively. Collectively, our findings highlight the potential role of immune cell phenotypes in the development of CD and UC as evidenced by data analysis from the FinnGen database. Therefore, the present study contributes to understanding the genetic basis of IBD and highlights the significance of immune cell phenotypes in disease pathogenesis.
},
year = {2025}
}
TY - JOUR T1 - Causal Role of Immune Cells in Inflammatory Bowel Disease: A Mendelian Randomization (MR) Study AU - Heng Shi AU - Qin Peng Y1 - 2025/04/29 PY - 2025 N1 - https://doi.org/10.11648/j.ijg.20250901.14 DO - 10.11648/j.ijg.20250901.14 T2 - International Journal of Gastroenterology JF - International Journal of Gastroenterology JO - International Journal of Gastroenterology SP - 25 EP - 31 PB - Science Publishing Group SN - 2640-169X UR - https://doi.org/10.11648/j.ijg.20250901.14 AB - The present Mendelian randomization study investigated the potential causal relationship between immunophenotypes and inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC). Results demonstrated that immunophenotypes, such as CD28 on CD39+ resting Treg and CD25 on IgD+ CD24− showed nominal significant protective effects on CD and UC, respectively. Conversely, specific immunophenotypes also exhibited nominal significant risk effects on CD and UC, including CD39 on CD39+ CD8br and IgD on IgD+ CD38dim, respectively. Collectively, our findings highlight the potential role of immune cell phenotypes in the development of CD and UC as evidenced by data analysis from the FinnGen database. Therefore, the present study contributes to understanding the genetic basis of IBD and highlights the significance of immune cell phenotypes in disease pathogenesis. VL - 9 IS - 1 ER -
Department of Gastroenterology, The Central Hospital of Shaoyang, Shaoyang, China
Department of Gastroenterology, The Central Hospital of Shaoyang, Shaoyang, China
Information