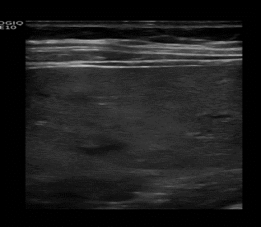
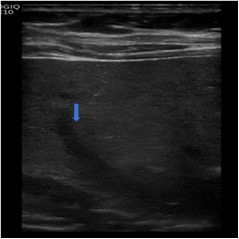
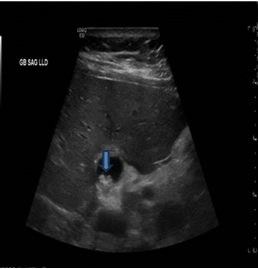
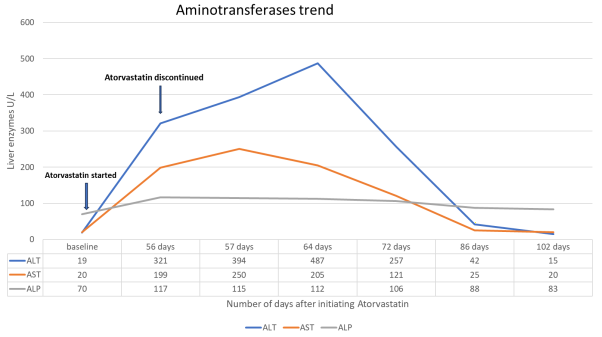
Background: Atorvastatin is a member of the class of cholesterol lowering drugs called statins, which works by inhibiting HMG-CoA reductase, an enzyme involved in cholesterol synthesis in the liver. Statins are used to reduce the risk of cardiovascular events in individuals who have risk factors or a history of cardiovascular disease. While atorvastatin is generally well-tolerated, like all statins, it can have some adverse effects, including Drug induced liver injury (DILI) which is rare and often dose related. However, there is scarcity of reports on symptomatic DILI occurring in patients on low dose statin and normal baseline liver function test. This case adds to the growing body of literature on the potential idiosyncratic, non-dose related adverse effects associated with atorvastatin therapy. Case report: A 69-year-old woman with history of Hypertension, Hyperlipidemia, Prediabetes, Non-Alcoholic Fatty Liver Disease (NAFLD) presented to her Primary care Physician (PCP) for regular follow up. Her Lipid panel in the last 1 year has been suboptimal with her Atherosclerotic Cardiovascular disease (ASCVD) risk score between 12.0-15.1% despite lifestyle modification. Patient was started on 10 mg of Atorvastatin daily after documenting normal baseline liver function test. Fifty-six days later, patient presented to the PCP’s office with symptoms of fatigue, nausea and, right upper abdominal pain for 3 days. She had right upper abdominal tenderness and was mildly icteric. Based on her PCPs suspicion for DILI, she was advised to discontinue atorvastatin and transferred to the emergency room for further evaluation. In the Emergency room her vitals remained stable. Liver Ultrasound showed normal sized liver with features of hepatic steatosis. Laboratory analysis showed elevated alanine aminotransferase (ALT) greater than 16 times Upper limit of normal (ULN), aspartate aminotransferase (AST) greater than 9 times ULN, while alkaline phosphatase (ALP) elevation was less than 2 times ULN suggesting hepatocellular pattern. She was seen by a hepatologist 1 week later and other etiologies of acute hepatitis were ruled out. Over the course of 4 weeks, her symptoms completely resolved and liver function tests continued to improve. Forty-six days after Atorvastatin was discontinued, her aminotransaminases returned to normal levels. Conclusion: Although DILI is usually dose dependent, this case emphasizes the need for constant monitoring of liver function test of patients on low dose statins including patients with normal baseline liver function test. Personalized medical approach involving validated predictive score for DILI may become increasingly important in tailoring statin therapy to minimize the risk of adverse effects.
| Published in | International Journal of Gastroenterology (Volume 8, Issue 1) |
| DOI | 10.11648/j.ijg.20240801.16 |
| Page(s) | 32-41 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Drug Induced Liver Injury, Hepatotoxicity, Idiosyncrasy, Statins
Tests (normal values) | Results |
|---|---|
Nuclear antibody screen with reflex IFA titer | Negative |
Immunoglobulin panel | Within normal limits |
Mitochondrial antibody qualitative | Negative |
Anti smooth muscle antibodies | Negative |
Anti liver-kidney microsome type 1antibodies | Negative |
Anti-nuclear antibody | Negative |
Anti ds-DNA | Negative |
Viral hepatitis A, B, C and E Serologies | Negative |
CMV (anti-CMV-IgM, anti-CMV-IgG) | Negative |
EBV (anti-EBV-IgM, anti-EBV-IgG) | Negative |
HSV (anti-HSV-IgM, anti-HSV-IgG) | Negative |
VZV (anti-VZV-IgM, anti-VZV-IgG) | Negative |
Echinococcus IGG | Negative |
Entamoeba Histolytica IGG | Negative |
C reactive protein (<0.8mg/dl) | <0.2mg/dl |
Ferritin (10-150 ng/ml) | 634ng/ml |
Amylase (<100U/L) | 99U/L |
Lipase (<60U/L) | 31U/L |
Creatinine Kinase (<200U/L) | 116 U/L |
Gastrointestinal infectious panel | Negative |
Stool for ova and parasite | Negative |
ALP | Alkaline Phosphatase |
ALT | Alanine Aminotransferase |
AST | Aspartate Aminotransferase |
ASCVD | Atherosclerotic Cardiovascular Disease |
DILI | Drug Induced Liver Injury |
GWAS | Genome-Wide Association Studies |
INR | International Normalized Ratio |
LDL | Low Density Lipoprotein |
NAFLD | Non-Alcoholic Fatty Liver Disease |
RUCAM | Roussel Uclaf Causality Assessment Method |
ULN | Upper Limit of Normal |
| [1] | Ward NC, Watts GF, Eckel RH. Statin Toxicity: Mechanistic Insights and Clinical Implications. Circ Res [Internet]. 2019 Jan 18 [cited 2023 Feb 6]; 124(2): 328–50. Available from: |
| [2] | Atorvastatin. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. 2021 Dec 1 [cited 2023 Feb 6]; Available from: |
| [3] |
Salami JA, Warraich H, Valero-Elizondo J, Spatz ES, Desai NR, Rana JS, et al. National Trends in Statin Use and Expenditures in the US Adult Population From 2002 to 2013: Insights From the Medical Expenditure Panel Survey. JAMA Cardiol [Internet]. 2017 Jan 1 [cited 2023 Jul 25]; 2(1): 56–65. Available from:
https://jamanetwork.com/journals/jamacardiology/fullarticle/2583425 |
| [4] |
Oesterle A, Laufs U, Liao JK. Pleiotropic Effects of Statins on the Cardiovascular System. Circ Res [Internet]. 2017 Jan 6 [cited 2023 Jul 29]; 120(1): 229–43. Available from:
https://www.ahajournals.org/doi/abs/10.1161/CIRCRESAHA.116.308537 |
| [5] | USPSTF Releases Updated Statin Guidelines For Primary Prevention of CVD - American College of Cardiology [Internet]. [cited 2023 Aug 1]. Available from: |
| [6] |
Virani SS, Smith SC, Stone NJ, Grundy SM. Secondary Prevention for Atherosclerotic Cardiovascular Disease: Comparing Recent US and European Guidelines on Dyslipidemia. Circulation [Internet]. 2020 Apr 7 [cited 2023 Aug 1]; 141(14): 1121–3. Available from:
https://www.ahajournals.org/doi/abs/10.1161/CIRCULATIONAHA.119.044282 |
| [7] | Grundy SM, Feingold KR. Guidelines for the Management of High Blood Cholesterol. Endotext [Internet]. 2022 May 28 [cited 2024 Jan 1]; Available from: |
| [8] |
Statin Safety and Adverse Events - American College of Cardiology [Internet]. [cited 2023 Aug 1]. Available from:
https://www.acc.org/latest-in-cardiology/articles/2018/12/12/07/23/statin-safety-and-adverse-events |
| [9] | Andrade RJ, Chalasani N, Björnsson ES, Suzuki A, Kullak-Ublick GA, Watkins PB, et al. Drug-induced liver injury. Nat Rev Dis Primers [Internet]. 2019 Dec 1 [cited 2023 Aug 4]; 5(1). Available from: |
| [10] | Teschke R, Schulze J, Eickhoff A, Danan G. Molecular Sciences Drug Induced Liver Injury: Can Biomarkers Assist RUCAM in Causality Assessment? [cited 2023 Aug 4]; Available from: |
| [11] | Fontana RJ, Liou I, Reuben A, Suzuki A, Fiel MI, Lee W, et al. AASLD practice guidance on drug, herbal, and dietary supplement-induced liver injury. Hepatology [Internet]. 2023 Mar 1 [cited 2023 Aug 4]; 77(3): 1036–65. Available from: |
| [12] | Chalasani NP, Maddur H, Russo MW, Wong RJ, Reddy KR. ACG Clinical Guideline: Diagnosis and Management of Idiosyncratic Drug-Induced Liver Injury. American Journal of Gastroenterology [Internet]. 2021 May 1 [cited 2023 Aug 4]; 116(5): 878–98. Available from: |
| [13] | Li X, Tang J, Mao Y. Incidence and risk factors of drug-induced liver injury. Liver International. 2022 Aug 1; 42(9): 1999–2014. |
| [14] | Drug-induced liver injury - UpToDate [Internet]. [cited 2023 Aug 5]. Available from: |
| [15] | Björnsson ES. Hepatotoxicity of statins and other lipid-lowering agents. Liver International [Internet]. 2017 Feb 1 [cited 2023 Aug 5]; 37(2): 173–8. Available from: |
| [16] | Björnsson ES. Hepatotoxicity by Drugs: The Most Common Implicated Agents. Int J Mol Sci [Internet]. 2016 Feb 6 [cited 2023 Aug 5]; 17(2). Available from: |
| [17] | Merli M, Bragazzi MC, Giubilo F, Callea F, Attili AF, Alvaro D. Atorvastatin-induced prolonged cholestasis with bile duct damage. Clin Drug Investig [Internet]. 2010 [cited 2023 Jan 31]; 30(3): 205–9. Available from: |
| [18] | Björnsson E, Jacobsen EI, Kalaitzakis E. Hepatotoxicity associated with statins: Reports of idiosyncratic liver injury post-marketing. J Hepatol. 2012 Feb 1; 56(2): 374–80. |
| [19] | Fisher K, Vuppalanchi R, Saxena R. Drug-Induced Liver Injury. Arch Pathol Lab Med [Internet]. 2015 Jul 1 [cited 2023 Sep 9]; 139(7): 876–87. Available from: |
| [20] | Khan AA, Ahmed S, Mohammed A, Elzouki ANY, Khan AA, Ahmed S, et al. Autoimmune-like Drug-induced Liver Injury Caused by Atorvastatin and Demonstration of the Safety Profile of Pravastatin: A Case Report and Literature Review. Cureus Journal of Medical Science [Internet]. 2020 Mar 17 [cited 2023 Feb 2]; 12(3). Available from: |
| [21] |
Garcia-Cortes M, Robles-Diaz M, Stephens C, Ortega-Alonso A, Lucena MI, Andrade RJ. Drug induced liver injury: an update. Archives of Toxicology 2020 94: 10 [Internet]. 2020 Aug 27 [cited 2023 Aug 25]; 94(10): 3381–407. Available from:
https://link.springer.com/article/10.1007/s00204-020-02885-1 |
| [22] | Bettega M, Miname MH, Rocha VZ, Dias R, Filho S, Rizerio B. STATIN-INDUCED HEPATITIS IN A SECONDARY PREVENTION PATIENT WITH SEVERE HYPERCHOLESTEROLEMIA. J Am Coll Cardiol [Internet]. 2017 Mar 21 [cited 2023 Feb 1]; 69(11): 2243. Available from: |
| [23] | Thotakura S, Singh A, Khera K, Chauhan S, Devasia T. Atorvastatin-Induced Hepatotoxicity, Increased by Clopidogrel Stress on CYP450 Enzyme: Understanding the Mechanism through a Case. J Appl Pharm Sci [Internet]. 2018 Apr 29 [cited 2023 Feb 1]; 8(4): 168–70. Available from: |
| [24] | Teschke R. Idiosyncratic DILI: Analysis of 46,266 Cases Assessed for Causality by RUCAM and Published From 2014 to Early 2019. Front Pharmacol [Internet]. 2019 Jul 23 [cited 2023 Aug 12]; 10: 730. Available from: |
| [25] |
Use of statins in patients with liver disease - Minerva Gastroenterologica e Dietologica 2014 March; 60(1): 15-24 - Minerva Medica - Journals [Internet]. [cited 2023 Sep 9]. Available from:
https://www.minervamedica.it/en/journals/gastroenterology/article.php?cod=R08Y2014N01A0015 |
| [26] | Njoku DB. Drug-Induced Hepatotoxicity: Metabolic, Genetic and Immunological Basis. Int J Mol Sci [Internet]. 2014 Apr 22 [cited 2023 Sep 9]; 15(4): 6990. Available from: |
| [27] | Averbukh LD, Turshudzhyan A, Wu DC, Wu GY. Statin-induced Liver Injury Patterns: A Clinical Review. J Clin Transl Hepatol [Internet]. 2022 Jun 6 [cited 2023 Sep 1]; 10(3): 543. Available from: |
| [28] | Roussel Uclaf Causality Assessment Method (RUCAM) in Drug Induced Liver Injury. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. 2019 May 4 [cited 2023 Oct 8]; Available from: |
| [29] | Tillmann HL, Suzuki A, Barnhart HX, Serrano J, Rockey DC. Tools for causality assessment in drug-induced liver disease. Curr Opin Gastroenterol. 2019 May 1[cited 2023 Aug 25]; 35(3): 183-190. Available from: |
| [30] | Francis P, Navarro VJ. Drug-Induced Hepatotoxicity. StatPearls [Internet]. 2022 Nov 11 [cited 2023 Sep 9]; Available from: |
| [31] | Onfiani G, Nascimbeni F, Carubbi F. A case of statin-induced liver injury with positive rechallenge with a second statin. Is there a class effect? J Basic Clin Physiol Pharmacol [Internet]. 2021 Nov 1 [cited 2023 Aug 27]; 32(6): 1151–5. Available from: |
| [32] | Carrascosa MF, Salcines-Caviedes JR, Lucena MI, Andrade RJ. Acute liver failure following atorvastatin dose escalation: is there a threshold dose for idiosyncratic hepatotoxicity? J Hepatol [Internet]. 2015 Mar 1 [cited 2023 Aug 27]; 62(3): 751–2. Available from: |
| [33] | Sikka P, Kapoor S, Saxena K. Statin Hepatotoxicity: Is it a Real Concern? Heart Views [Internet]. 2011 [cited 2023 Feb 6]; 12(3): 104. Available from: |
| [34] | Rzouq FS, Volk ML, Hatoum HH, Talluri SK, Mummadi RR, Sood GK. Hepatotoxicity fears contribute to underutilization of statin medications by primary care physicians. Am J Med Sci [Internet]. 2010 [cited 2023 Feb 6]; 340(2): 89–93. Available from: |
| [35] | Toth PP, Banach M. Statins: Then and Now. Methodist Debakey Cardiovasc J [Internet]. 2019 Jan 1 [cited 2023 Aug 10]; 15(1): 23. Available from: |
| [36] | Jose J. Statins and its hepatic effects: Newer data, implications, and changing recommendations. J Pharm Bioallied Sci [Internet]. 2016 Jan 1 [cited 2023 Sep 9]; 8(1): 23. Available from: |
| [37] | Hassan A, Fontana RJ. The diagnosis and management of idiosyncratic drug-induced liver injury. Liver International [Internet]. 2019 Jan 1 [cited 2023 Sep 9]; 39(1): 31–41. Available from: |
| [38] | Howell LS, Ireland L, Park BK, Goldring CE. MiR-122 and other microRNAs as potential circulating biomarkers of drug-induced liver injury. Expert Rev Mol Diagn [Internet]. 2018 Jan 2 [cited 2023 Aug 25]; 18(1): 47–54. Available from: |
| [39] | Cirulli ET, Nicoletti P, Abramson K, Andrade RJ, Bjornsson ES, Chalasani N, et al. A Missense Variant in PTPN22 is a Risk Factor for Drug-induced Liver Injury. Gastroenterology [Internet]. 2019 May 1 [cited 2023 Oct 16]; 156(6): 1707-1716.e2. Available from: |
| [40] | Real M, Barnhill MS, Higley C, Rosenberg J, Lewis JH. Drug-Induced Liver Injury: Highlights of the Recent Literature. Drug Saf [Internet]. 2019 Mar 7 [cited 2023 Sep 2]; 42(3): 365–87. Available from: |
| [41] | Dean L, Kane M. Allopurinol Therapy and HLA-B*58:01 Genotype. Medical Genetics Summaries [Internet]. 2020 Dec 9 [cited 2023 Oct 19]; Available from: |
| [42] | Dean L. Abacavir Therapy and HLA-B*57:01 Genotype. Medical Genetics Summaries [Internet]. 2018 Apr 18 [cited 2023 Oct 18]; Available from: |
| [43] | Marques AC, Busanello ENB, de Oliveira DN, Catharino RR, Oliveira HCF, Vercesi AE. Coenzyme Q10 or Creatine Counteract Pravastatin-Induced Liver Redox Changes in Hypercholesterolemic Mice. Front Pharmacol [Internet]. 2018 Jun 27 [cited 2023 Aug 31]; 9(JUN). Available from: |
| [44] | Golomb BA, Evans MA. Statin adverse effects : a review of the literature and evidence for a mitochondrial mechanism. Am J Cardiovasc Drugs [Internet]. 2008 [cited 2023 Sep 1]; 8(6): 373–418. Available from: |
| [45] | Fontana RJ, Watkins PB, Bonkovsky HL, Chalasani N, Davern T, Serrano J, et al. Drug-Induced Liver Injury Network (DILIN) Prospective Study: Rationale, Design and Conduct. Drug safety: an international journal of medical toxicology and drug experience [Internet]. 2009 [cited 2023 Sep 9]; 32(1): 55. Available from: |
APA Style
Adetiloye, A., Badero, O. (2024). Rare Clinically Significant Idiosyncratic Drug Induced Liver Injury Caused by Low Dose Atorvastatin: Time for a New Approach to Surveillance and Risk Identification. International Journal of Gastroenterology, 8(1), 32-41. https://doi.org/10.11648/j.ijg.20240801.16
ACS Style
Adetiloye, A.; Badero, O. Rare Clinically Significant Idiosyncratic Drug Induced Liver Injury Caused by Low Dose Atorvastatin: Time for a New Approach to Surveillance and Risk Identification. Int. J. Gastroenterol. 2024, 8(1), 32-41. doi: 10.11648/j.ijg.20240801.16
AMA Style
Adetiloye A, Badero O. Rare Clinically Significant Idiosyncratic Drug Induced Liver Injury Caused by Low Dose Atorvastatin: Time for a New Approach to Surveillance and Risk Identification. Int J Gastroenterol. 2024;8(1):32-41. doi: 10.11648/j.ijg.20240801.16
@article{10.11648/j.ijg.20240801.16,
author = {Adebola Adetiloye and Olurotimi Badero},
title = {Rare Clinically Significant Idiosyncratic Drug Induced Liver Injury Caused by Low Dose Atorvastatin: Time for a New Approach to Surveillance and Risk Identification
},
journal = {International Journal of Gastroenterology},
volume = {8},
number = {1},
pages = {32-41},
doi = {10.11648/j.ijg.20240801.16},
url = {https://doi.org/10.11648/j.ijg.20240801.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20240801.16},
abstract = {Background: Atorvastatin is a member of the class of cholesterol lowering drugs called statins, which works by inhibiting HMG-CoA reductase, an enzyme involved in cholesterol synthesis in the liver. Statins are used to reduce the risk of cardiovascular events in individuals who have risk factors or a history of cardiovascular disease. While atorvastatin is generally well-tolerated, like all statins, it can have some adverse effects, including Drug induced liver injury (DILI) which is rare and often dose related. However, there is scarcity of reports on symptomatic DILI occurring in patients on low dose statin and normal baseline liver function test. This case adds to the growing body of literature on the potential idiosyncratic, non-dose related adverse effects associated with atorvastatin therapy. Case report: A 69-year-old woman with history of Hypertension, Hyperlipidemia, Prediabetes, Non-Alcoholic Fatty Liver Disease (NAFLD) presented to her Primary care Physician (PCP) for regular follow up. Her Lipid panel in the last 1 year has been suboptimal with her Atherosclerotic Cardiovascular disease (ASCVD) risk score between 12.0-15.1% despite lifestyle modification. Patient was started on 10 mg of Atorvastatin daily after documenting normal baseline liver function test. Fifty-six days later, patient presented to the PCP’s office with symptoms of fatigue, nausea and, right upper abdominal pain for 3 days. She had right upper abdominal tenderness and was mildly icteric. Based on her PCPs suspicion for DILI, she was advised to discontinue atorvastatin and transferred to the emergency room for further evaluation. In the Emergency room her vitals remained stable. Liver Ultrasound showed normal sized liver with features of hepatic steatosis. Laboratory analysis showed elevated alanine aminotransferase (ALT) greater than 16 times Upper limit of normal (ULN), aspartate aminotransferase (AST) greater than 9 times ULN, while alkaline phosphatase (ALP) elevation was less than 2 times ULN suggesting hepatocellular pattern. She was seen by a hepatologist 1 week later and other etiologies of acute hepatitis were ruled out. Over the course of 4 weeks, her symptoms completely resolved and liver function tests continued to improve. Forty-six days after Atorvastatin was discontinued, her aminotransaminases returned to normal levels. Conclusion: Although DILI is usually dose dependent, this case emphasizes the need for constant monitoring of liver function test of patients on low dose statins including patients with normal baseline liver function test. Personalized medical approach involving validated predictive score for DILI may become increasingly important in tailoring statin therapy to minimize the risk of adverse effects.
},
year = {2024}
}
TY - JOUR T1 - Rare Clinically Significant Idiosyncratic Drug Induced Liver Injury Caused by Low Dose Atorvastatin: Time for a New Approach to Surveillance and Risk Identification AU - Adebola Adetiloye AU - Olurotimi Badero Y1 - 2024/06/06 PY - 2024 N1 - https://doi.org/10.11648/j.ijg.20240801.16 DO - 10.11648/j.ijg.20240801.16 T2 - International Journal of Gastroenterology JF - International Journal of Gastroenterology JO - International Journal of Gastroenterology SP - 32 EP - 41 PB - Science Publishing Group SN - 2640-169X UR - https://doi.org/10.11648/j.ijg.20240801.16 AB - Background: Atorvastatin is a member of the class of cholesterol lowering drugs called statins, which works by inhibiting HMG-CoA reductase, an enzyme involved in cholesterol synthesis in the liver. Statins are used to reduce the risk of cardiovascular events in individuals who have risk factors or a history of cardiovascular disease. While atorvastatin is generally well-tolerated, like all statins, it can have some adverse effects, including Drug induced liver injury (DILI) which is rare and often dose related. However, there is scarcity of reports on symptomatic DILI occurring in patients on low dose statin and normal baseline liver function test. This case adds to the growing body of literature on the potential idiosyncratic, non-dose related adverse effects associated with atorvastatin therapy. Case report: A 69-year-old woman with history of Hypertension, Hyperlipidemia, Prediabetes, Non-Alcoholic Fatty Liver Disease (NAFLD) presented to her Primary care Physician (PCP) for regular follow up. Her Lipid panel in the last 1 year has been suboptimal with her Atherosclerotic Cardiovascular disease (ASCVD) risk score between 12.0-15.1% despite lifestyle modification. Patient was started on 10 mg of Atorvastatin daily after documenting normal baseline liver function test. Fifty-six days later, patient presented to the PCP’s office with symptoms of fatigue, nausea and, right upper abdominal pain for 3 days. She had right upper abdominal tenderness and was mildly icteric. Based on her PCPs suspicion for DILI, she was advised to discontinue atorvastatin and transferred to the emergency room for further evaluation. In the Emergency room her vitals remained stable. Liver Ultrasound showed normal sized liver with features of hepatic steatosis. Laboratory analysis showed elevated alanine aminotransferase (ALT) greater than 16 times Upper limit of normal (ULN), aspartate aminotransferase (AST) greater than 9 times ULN, while alkaline phosphatase (ALP) elevation was less than 2 times ULN suggesting hepatocellular pattern. She was seen by a hepatologist 1 week later and other etiologies of acute hepatitis were ruled out. Over the course of 4 weeks, her symptoms completely resolved and liver function tests continued to improve. Forty-six days after Atorvastatin was discontinued, her aminotransaminases returned to normal levels. Conclusion: Although DILI is usually dose dependent, this case emphasizes the need for constant monitoring of liver function test of patients on low dose statins including patients with normal baseline liver function test. Personalized medical approach involving validated predictive score for DILI may become increasingly important in tailoring statin therapy to minimize the risk of adverse effects. VL - 8 IS - 1 ER -
Department of Internal Medicine, Montefiore Medical Group, New York, USA
Information