Abstract
To explore the application of left ventricular (LV) stratified strain in evaluating early systolic dysfunction in diabetes patients with and without LV remodeling by using two-dimensional speckle tracking echocardiography (2DSTE), This study included 35 diabetes patients and 25 healthy individuals. All participants completed echography by GE Vivid E9 ultrasound system. The diabetes patients were subdivided based on relative wall thickness into normal LV geometry group and LV remodeling group. The EchoPAC offline workstation was used to analyze LV myocardial longitudinal layer-specific strain. Our results showed that compared to the control group, the absolute values of longitudinal strain in the endocardial, mid-myocardial, and epicardial layers of the 3-chamber view, the epicardial layer of the 4-chamber view, as well as the average longitudinal strain of the mid-myocardial and epicardial layers across all three views, were significantly decreased in the diabetes group (P < 0.05). Compared to the control group, both the normal LV geometry and LV remodeling subgroups showed significantly reduced absolute values of longitudinal strain in the epicardial layer of the 3-chamber and 4-chamber views, and in the average epicardial strain across all three views (P < 0.05), with the most pronounced changes observed in the LV remodeling group. Furthermore, compared to the control group, the LV remodeling subgroup exhibited significantly reduced absolute values of longitudinal strain in the endocardial and mid-myocardial layers of the 3-chamber view, the endocardial layer of the 4-chamber view, and the average mid-myocardial strain across all three views (P < 0.05). A significant decrease in the absolute value of epicardial longitudinal strain in the 3-chamber view was also found in the LV remodeling group compared to the normal LV geometry group (P < 0.05). The study reveals that in diabetes patients with either normal LV geometry or LV remodeling, impairment of epicardial longitudinal strain in the 3-chamber and 4-chamber views, as well as the average epicardial strain, occurs earlier. In diabetes patients with LV remodeling, longitudinal strain in the endocardial and mid-myocardial layers of the 3-chamber view, the endocardial layer of the 4-chamber view, and the average mid-myocardial strain were the most sensitively impaired parameters. Additionally, the impairment of myocardial longitudinal strain was most pronounced in the apical 3-chamber view.
Keywords
Echocardiography, Two-dimensional Speckle Tracking Echocardiography, Diabetes Mellitus,
Left Ventricular Layer-specific Strain, Left Ventricular Function
1. Introduction
Diabetes Mellitus (DM) is a disease with significant global, showing a pronounced increasing trend in prevalence worldwide. It is projected that by 2035, the global number of people living with diabetes will exceed 783.2 million
| [1] | Hong, Sun, Pouya, Saeedi, Suvi, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. [J]. Diabetes Res Clin Pract, 2021, 183: 109119.
https://doi.org/10.1016/j.diabres.2021.109119 |
[1]
. As an incurable disease, DM begins with the high glucose toxicity that leads to various complications, which not only cause serious physical damage to patients but also impose a considerable burden on existing healthcare resources and the economy. Among the microvascular and macrovascular complications of diabetes, the incidence of diabetic cardiomyopathy (DCM) reaches 15%-20%. DCM is the primary and most prevalent disease leading to decreased myocardial cell function, increased cardiac morbidity, and elevated mortality
| [2] | Bhagyalakshmi, Balakrishnan, Raghu Chandrashekar, et al. Hyperglycaemia to heart failure: molecular pathophysiology, clinical manifestations, and novel therapeutic targets for diabetic cardiomyopathy. [J]. Arch Physiol Biochem, 2025, undefined: 1-14. https://doi.org/10.1080/13813455.2025.2567336 |
[2]
. As a major complication of diabetes, DCM refers to the impairment of myocardial contraction and/or diastolic function in the presence of diabetes, independent of coronary artery disease and hypertension. This diabetes-related myocardial pathology can lead to a significant increase in the risk of heart failure and death. According to statistics, the risk of developing heart failure in individuals with DM is 4-5 times higher than in non-diabetic populations. The five-year mortality rate for diagnosed DCM patients with heart failure is as high as 50%, a prognosis comparable to that of malignant tumors
| [2] | Bhagyalakshmi, Balakrishnan, Raghu Chandrashekar, et al. Hyperglycaemia to heart failure: molecular pathophysiology, clinical manifestations, and novel therapeutic targets for diabetic cardiomyopathy. [J]. Arch Physiol Biochem, 2025, undefined: 1-14. https://doi.org/10.1080/13813455.2025.2567336 |
| [3] | W B, Kannel, M, et al. Role of diabetes in congestive heart failure: the Framingham study. [J]. Am J Cardiol, 1974, 34: 29-34. https://doi.org/10.1016/0002-9149(74)90089-7 |
[2, 3]
. The damage inflicted by DCM on the heart involves complex processes affecting metabolism, structure, microvasculature, and nerves. Through mechanisms such as metabolic disturbances and energy deprivation, myocardial fibrosis and interstitial remodeling, microvascular dysfunction and endothelial dysfunction, and cardiac autonomic neuropathy, these factors collectively ultimately lead to impaired left ventricular function and structure
| [2] | Bhagyalakshmi, Balakrishnan, Raghu Chandrashekar, et al. Hyperglycaemia to heart failure: molecular pathophysiology, clinical manifestations, and novel therapeutic targets for diabetic cardiomyopathy. [J]. Arch Physiol Biochem, 2025, undefined: 1-14. https://doi.org/10.1080/13813455.2025.2567336 |
[2]
. Left ventricular functional damage initially and primarily manifests as diastolic dysfunction, followed by the emergence of impaired left ventricular systolic function. This progression is primarily driven by myocardial fibrosis, increased stiffness, and energy metabolism disorders. As the condition advances, it ultimately evolves into heart failure
| [4] | Mohapradeep, Mohan, Adel, et al. Left Ventricular Hypertrophy in Diabetic Cardiomyopathy: A Target for Intervention. [J]. Front Cardiovasc Med, 2021, 8: 746382.
https://doi.org/10.3389/fcvm.2021.746382 |
[4]
.
Therefore, the early detection of impaired left ventricular function in diabetes patients and timely intervention are crucial for alleviating patient suffering and improving prognosis. Echocardiography is recommended as the primary method for cardiac function monitoring. While conventional left ventricular ejection fraction (LVEF) is one of the most used indicators for assessing cardiac function, changes in LVEF typically manifest only in the advanced stages of the disease, making it unsuitable for evaluating early stage left ventricular systolic dysfunction.
Two-Dimensional Speckle Tracking Echocardiography (2DSTE) is a technique based on two-dimensional ultrasound imaging that utilizes acoustic speckle tracking to observe displacement changes in myocardial segments within the region of interest. Due to its advantages—being unaffected by the angle between the ultrasound beam and wall motion, lacking angle dependency, and offering greater objectivity—2DSTE has been applied in assessing early left ventricular systolic function, evaluating the effectiveness and rationale of patient treatment plans, and is now widely used in diagnostic research for various cardiac function impairment diseases
| [5] | Victor, Mor-Avi, Roberto M, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. [J].J Am Soc Echocardiogr, 2011, 24: 277-313. https://doi.org/10.1016/j.echo.2011.01.015 |
| [6] | Elizabeth, Potter, Thomas H, et al. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. [J]. JACC Cardiovasc Imaging, 2018, 11: 260-274.
https://doi.org/10.1016/j.jcmg.2017.11.017 |
[5, 6]
. For instance, left ventricular global longitudinal strain (GLS) is regarded as a sensitive indicator for evaluating cardiac systolic function and can detect changes in cardiac systolic function during the subclinical stage
. However, GLS reflects the average strain of the entire left ventricle and is not sufficiently sensitive for detecting very early-stage pathologies involving regional, heterogeneous myocardial damage, or for localizing impairment in specific myocardial layers
| [5] | Victor, Mor-Avi, Roberto M, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. [J].J Am Soc Echocardiogr, 2011, 24: 277-313. https://doi.org/10.1016/j.echo.2011.01.015 |
[5]
. Consequently, left ventricular longitudinal layer-specific strain has emerged to overcome this limitation. It can identify the earliest and most subtle myocardial damage, precisely localize the affected myocardial layer, and reflect different layer-specific strain impairment patterns that suggest distinct pathophysiological mechanisms. This provides deeper insights for clinical diagnosis with high sensitivity and specificity
| [8] | Darae, Kim, Chi Young, et al. Differences in left ventricular functional adaptation to arterial stiffness and neurohormonal activation in patients with hypertension: a study with two-dimensional layer-specific speckle tracking echocardiography. [J]. Clin Hypertens, 2017, 23: 21.
https://doi.org/10.1186/s40885-017-0078-9 |
[8]
. Recent studies have found that left ventricular longitudinal layer-specific strain can more sensitively detect early myocardial damage in various conditions, such as dilated cardiomyopathy, hypertrophic cardiomyopathy, hypertension, and septic cardiomyopathy
| [9] | Otto A, Smiseth, et al. Myocardial strain imaging: how useful is it in clinical decision making? [J]. Eur Heart J, 2015, 37: 1196-207. https://doi.org/10.1093/eurheartj/ehv529 |
| [10] | Patrick, Garceau, Shemy, et al. Evaluation of left ventricular relaxation and filling pressures in obstructive hypertrophic cardiomyopathy: comparison between invasive hemodynamics and two-dimensional speckle tracking. [J]. Echocardiography, 2012, 29: 934-42.
https://doi.org/10.1111/j.1540-8175.2012.01708.x |
| [11] | Ieva, Kažukauskienė, Giedrė, et al. Left ventricular global longitudinal strain predicts elevated cardiac pressures and poor clinical outcomes in patients with non-ischemic dilated cardiomyopathy. [J]. Cardiovasc Ultrasound, 2021, 19: 21.
https://doi.org/10.1186/s12947-021-00254-1 |
| [12] | Wei-Ting, Chang, Wen-Huang, et al. Left ventricular global longitudinal strain is independently associated with mortality in septic shock patients. [J]. Intensive Care Med, 2015, 41: 1791-9. https://doi.org/10.1007/s00134-015-3970-3 |
| [13] | Despina-Manuela, Toader, Alina, et al. Layer-Specific Strain Analysis in Patients with Dilated Cardiomyopathy. [J]. Biomedicines, 2025, 13:
https://doi.org/10.3390/biomedicines13010011 |
[9-13]
. However, research on early layer-specific myocardial impairment in diabetes using this technique remains relatively limited. Whether the impact on left ventricular layer-specific strain differs between diabetes patients with and without left ventricular remodeling is currently unknown.
Therefore, this study utilized the GE Vivid E9 ultrasound system with corresponding offline analysis workstations to perform 2DSTE on both the case and control groups. The aim was to investigate the value of LV layer-specific strain in assessing early cardiac dysfunction in diabetes patients. This approach enhances the understanding of the pathogenic mechanisms underlying DCM and provides a more sensitive and reliable clinical indicator for early detection, diagnosis, and treatment monitoring of this condition.
2. Methods
2.1. Study Design
A total of 35 patients with DM from the Department of Endocrinology at West China Hospital of Sichuan University were collected and included as the case group between June 2022 and March 2023. During the same period, 25 healthy individuals were recruited as the control group. Among the 35 diabetes patients, subgroups were further divided based on the presence or absence of left ventricular geometric pattern changes—specifically, relative wall thickness (RWT). The patients were categorized into two subgroups: the normal left ventricular geometry subgroup (RWT < 0.42) and the left ventricular remodeling subgroup (RWT ≥ 0.42)
| [14] | Helmut, Baumgartner, Judy, et al. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. [J]. J Am Soc Echocardiogr, 2017, 30: 372-392.
https://doi.org/10.1016/j.echo.2017.02.009 |
[14]
. Inclusion Criteria: (1) Diagnostic criteria for diabetes mellitus: according to the 2025 American Diabetes Association (ADA) diagnostic criteria
; (2) LVEF ≥ 55%; (3) Sinus rhythm during echocardiographic examination; (4) Agreement to participate in this study and provision of signed informed consent. Exclusion Criteria: (1) Presence of structural heart disease, valvular heart disease, arrhythmia, or other conditions that may cause cardiovascular disease; (2) LVEF < 55%; (3) Poor image quality affecting diagnosis. And the diagnosis of coronary heart disease, valvular disease, or cardiomyopathy integrate history, ECG, coronary CTA etc. A total of 6 participants were excluded due to poor ultrasound image quality. All the subjects of the study provided written informed consent.
2.2. Basic Clinical Data and Routine Echocardiography
Acquisition of Basic Clinical Data: basic clinical data, including age, sex, blood pressure, duration of diabetes, and glycated hemoglobin (HbA1c), were collected for all study subjects. Acquisition of Conventional Cardiac Ultrasound Data: Conventional echocardiographic images were acquired and data were measured using a GE Vivid E9 ultrasound diagnostic system with an M5Sc probe, with its frame rate adjusted to 1.5–4.6 MHz. The following parameters were collected for all subjects: left ventricular end-diastolic diameter (LVEDD), posterior wall end-diastolic diameter (PWDD), left ventricular end-diastolic volume (LVEDV), left ventricular ejection fraction (LVEF), RWT, and E/Em. RWT was calculated using the formula: RWT = (IVSd + LVPWd) / LVDd
| [14] | Helmut, Baumgartner, Judy, et al. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. [J]. J Am Soc Echocardiogr, 2017, 30: 372-392.
https://doi.org/10.1016/j.echo.2017.02.009 |
[14]
. After image acquisition from the apical four-chamber and two-chamber views, the left ventricular ejection fraction was calculated using the biplane Simpson's method.
2.3.2. DSTE Analysis
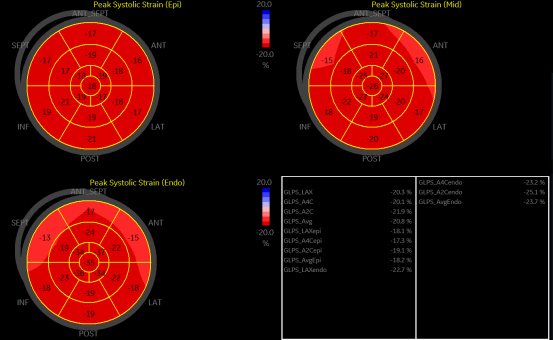
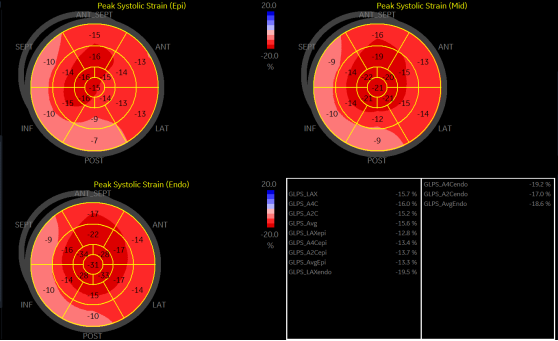
Two-dimensional images were acquired for all study subjects from the left ventricular apical four-chamber, three-chamber, and two-chamber views using an M5Sc probe (Vivid E9, with the probe frame rate adjusted to 1.5–4.6 MHz). All participants were instructed to hold their breath during image acquisition to ensure high-quality images. During image acquisition, electrocardiogram (ECG) was simultaneously recorded, and images covering 3-5 complete cardiac cycles were obtained. The frame rate was adjusted to 40–80 fps. After image collection, speckle tracking quantitative analysis was performed using an EchoPAC workstation (version 201). The left ventricular endocardium was tracked point-by-point sequentially in the apical three-chamber, four-chamber, and two-chamber view images. Simultaneously, based on the timing of aortic and mitral valve opening and closure, manual adjustments were made for segments with unsatisfactory tracking. After successfully tracking the 17 segments of the left ventricle, the subendocardial strain, mid-myocardial strain, and subepicardial strain for the different views, as well as the average subendocardial strain, mid-myocardial strain, and subepicardial strain across the three views, were automatically obtained. The analysis of LV layered longitudinal strain in the control group and the case group is shown in
Figure 1 and
Figure 2, respectively.
Figure 1. Displays the left ventricular layered longitudinal strain analyzed by two-dimensional speckle tracking in healthy individuals from the control group.
Figure 2. Displays the left ventricular layered longitudinal strain analyzed by two-dimensional speckle tracking in diabetes patients from the case group.
2.4. Statistical Analysis
All statistical analyses were performed using SPSS version 26.0. Continuous variables were compared between the case group and normal control group using independent samples t-tests or Mann-Whitney U tests, while one-way ANOVA or Kruskal-Wallis tests were employed for multi-group comparisons. Categorical data were analyzed using the Chi-square test. A two-tailed P-value < 0.05 was considered statistically significant. For intra-observer reproducibility assessment, 40% of subjects were randomly selected for repeated analyses of the same images were performed at different time points. Intraclass correlation coefficient (ICC) was used to evaluate the reproducibility of left ventricular mean mid-myocardial longitudinal strain measurements.
3. Results
3.1. Comparison of General Clinical Data Between the DM Group and the Control Group
Table 1. Comparison of basic clinical data between the case group and the control group.
| Control group (n=25) | Case group (n=35) | Normal left ventricular geometry subgroup (n=18) | Left ventricular remodeling subgroup (n=17) |
Age (years) | 49.89±8.26 | 50.29±8.64 | 51±8.64 | 48.71±6.26 |
Male/female (case) | 10/15 | 20/15 | 10/8 | 10/7 |
BSA (m2) | 1.94±0.14 | 2.06±0.15 | 2.05±0.04 | 2.07±0.05# |
HbA1c (%) | 5.6±0.5 | 6.41±1.00* | 6.63±0.54** | 6.38±0.74# |
systolic blood pressure (mmHg) | 125.84±8.18 | 132.54±9.42* | 131.28±5.61** | 133.88±4.44# |
diastolic blood pressure (mmHg) | 75.68±4.76 | 88.39±4.43 | 87.33±4.42 | 89.94±3.13# |
duration of diabetes (years) | - | 3.66±1.75 | 2.44±1.10 | 4.88±1.41 |
Heart rate (beats/minute) | 69.68±9.26 | 74.17±9.64 | 72.33±4.94 | 76.12±6.07 |
Data is represented as the mean ± SD or as numbers.
Body Surface Area (BSA); Glycated Hemoglobin (HbA1c); Diabetes Mellitus (DM).
* P < 0.05 for case group vs. control group; ** P < 0.05 for normal left ventricular geometry subgroup vs. control group; # P < 0.05 for left ventricular remodeling subgroup vs. control group.
As shown in
Table 1, compared to the control group, the case group showed significantly higher levels of glycated hemoglobin (HbA1c) and systolic blood pressure, with the differences being statistically significant (P < 0.05). In contrast, no statistically significant differences were observed between the case group and the control group in terms of age, sex, body surface area (BSA), diastolic blood pressure, or heart rate (P > 0.05). Based on the presence or absence of left ventricular remodeling, the DM group was further divided into a normal left ventricular geometry subgroup and a left ventricular remodeling subgroup. Compared to the control group, both the normal left ventricular geometry subgroup and the left ventricular remodeling subgroup exhibited significantly elevated glycated hemoglobin and systolic blood pressure, with these differences being statistically significant (P < 0.05). Additionally, compared to the control group, the left ventricular remodeling subgroup showed statistically significant differences in body surface area and diastolic blood pressure (P < 0.05). However, no statistically significant differences were observed among the groups in terms of age, sex, body surface area, glycated hemoglobin, systolic blood pressure, diastolic blood pressure, duration of diabetes, or heart rate (P > 0.05).
3.2. Comparison of Conventional Echocardiographic Parameters Between the Case Group and the Control Group
Table 2. Comparison of conventional ultra-sound parameters between the case group and the control group.
| Control group (n =25) | Case group (n=35) | Normal left ventricular geometry subgroup (n=18) | Left ventricular remodeling subgroup (n=17) |
LVEDD (mm) | 46.24±3.24 | 46.84±8.34 | 47.67±3.20 | 46.08±3.34 |
LVEDV (mL) | 100.32±15.06 | 102.36±15.02 | 104.44±15.19 | 100.35±19.31 |
IVST (mm) | 9.16±1.14 | 9.98±1.22* | 9.78±1.22**## | 11.65±1.06# |
LVPWT (mm) | 8.36±0.76 | 9.11±0.77 | 8.83±0.79 | 9.41±1.00# |
LVEF (%) | 67.24±4.92 | 66.60±0.32 | 65.78±6.38 | 67.29±4.42 |
RWT | 0.38±0.05 | 0.42±0.14 | 0.39±0.03## | 0.46±0.04# |
E/Em | 10.64±2.36 | 11.5±2.76 | 11.33±2.27 | 11.82±3.43 |
Data is represented as the mean ± SD or as numbers.
Left Ventricular End-Diastolic Diameter (LVEDD); Left Ventricular End-Diastolic Volume (LVEDV); Interventricular Septal Thickness (IVST); Left Ventricular Posterior Wall Thickness (LVPWT); Left Ventricular Ejection Fraction (LVEF); Relative Wall Thickness (RWT); E: Mitral Early Diastolic Inflow Velocity; Em: Early Diastolic Mitral Annular Tissue Velocity.
* P <0.05 for case group vs. control group; **P <0.05 for normal left ventricular geometry subgroup vs. control group; #P <0.05 for left ventricular remodeling subgroup vs. control group; ##P <0.05 for left ventricular remodeling subgroup vs. normal left ventricular geometry subgroup.
As shown in
Table 2, compared with the control group, IVST in the case group was thickened, and the difference was statistically significant (P < 0.05). In contrast, no statistically significant differences were observed in LVEDD, LVEDV, LVPWT, LVEF, RWT between the two groups (P > 0.05). In the subgroup analysis, we found that compared to the control group, both the normal left ventricular geometry subgroup and the left ventricular remodeling subgroup showed IVST with the differences being statistically significant (P < 0.05). Furthermore, the left ventricular remodeling subgroup demonstrated a significant increase in LVPWT, RWT compared to the control group, and these differences were statistically significant (P < 0.05). More importantly, when compared to the normal left ventricular geometry subgroup, the left ventricular remodeling subgroup exhibited significantly greater IVST and RWT and these differences were statistically significant (P < 0.05).
3.3. Comparison of Left Ventricular Layered Longitudinal Strain Between the Case Group and Control Group
As shown in
Table 3, compared to the control group, the case group demonstrated a statistically significant decrease (P < 0.05) in the absolute values of left ventricular longitudinal strain in the following layers and views: the subendocardial, mid-myocardial, and subepicardial layers of the three-chamber view; the subepicardial and mid-myocardial layers of the four-chamber view; and the average subepicardial strain. When compared to the control group, both the normal left ventricular geometry subgroup and the left ventricular remodeling subgroup showed a statistically significant reduction (P < 0.05) in the absolute values of left ventricular longitudinal strain in the subepicardial layer of the three-chamber view, the subepicardial layer of the four-chamber view, and the average subepicardial strain. Furthermore, the left ventricular remodeling subgroup also exhibited a significant decrease (P < 0.05) in the absolute values of strain in the following parameters compared to the control group: the subendocardial and mid-myocardial layers of the three-chamber view; the subendocardial layer of the four-chamber view; and the average mid-myocardial strain. Importantly, when compared to the normal left ventricular geometry subgroup, the left ventricular remodeling subgroup showed a statistically significant reduction (P < 0.05) in the absolute value of longitudinal strain specifically in the subepicardial layer of the three-chamber view.
Table 3. Comparison of the difference of left ventricular longitudinal strain between the case group and the control group.
| Control group (n=25) | Case group (n=35) | Normal left ventricular geometry subgroup (n=18) | Left ventricular remodeling subgroup (n=17) |
Three chamber view-endo | 23.35±2.88 | 21.48±3.60* | 21.90±2.88 | 19.41±3.56# |
Three chamber view-mid | 21.62±3.45 | 18.82±3.30* | 19.28±2.58 | 17.01±3.43# |
three-chamber view-epi | 20.45±3.26 | 16.40±3.02* | 18.03±2.38**## | 14.76±3.23# |
Four chamber view-endo | 21.98±4.31 | 19.00±3.86 | 20.43±3.24 | 18.80±2.02# |
Four chamber view-mid | 21.08±4.06 | 20.59±2.91 | 20.64±2.79 | 20.51±2.79 |
Four chamber view-epi | 21.13±3.84 | 16.04±2.66* | 16.45±2.51** | 14.08±1.43# |
two chamber view-endo | 24.16±3.62 | 22.98±3.66 | 23.70±3.82 | 22.58±3.60 |
two chamber view-mid | 21.98±4.04 | 20.53±3.19 | 20.78±3.39 | 20.17±3.08 |
two chamber view-epi | 21.86±3.73 | 20.09±2.88 | 20.82±3.08 | 19.18±2.72 |
Average endo-myocardium | 23.29±3.48 | 22.27±2.78 | 22.62±2.23 | 19.95±3.20 |
Average mid-myocardium | 21.48±3.15 | 18.77±2.49* | 19.98±1.97 | 17.72±1.48# |
Average epi-myocardium | 21.23±2.91 | 17.82±2.30 | 18.77±1.88** | 17.50±1.31# |
Data is represented as the mean ± SD or as numbers. All strain data in the table are absolute values of actual measurements.
* P <0.05 for case group vs. control group, **P <0.05 for normal left ventricular geometry group vs. control group, #P <0.05 for left ventricular remodeling group vs. control group; ##P <0.05 for left ventricular remodeling group vs. normal left ventricular geometry group.
3.4. Intra-observer Reproducibility Analysis
Intra-observer agreement was assessed in a randomly selected subset comprising 40% of the study participants. The same physician performed identical ultrasound examinations and strain analyses for these subjects at different time points. The two sets of measured values for the average mid-myocardial longitudinal strain obtained from each subject were used for the intra-observer reproducibility analysis, and the intraclass correlation coefficient (ICC) was calculated.
As shown in
Table 4, the resulting ICC value was 0.929 (95% CI: 0.846 to 0.968). An ICC value greater than 0.9 indicates excellent agreement between the two measurements taken by the same physician for the same subject in this study.
Table 4. Results of Intraclass Correlation Coefficient (ICC) for Intra-observer Agreement.
Two-way mixed-effects model, absolute agreement | ICC | 95% CI |
Single-Measure ICC (A, 1) | 0.929 | 0.846 ~ 0.968 |
Average-Measure ICC (A, k) | 0.963 | 0.917 ~ 0.984 |
A denotes Absolute Agreement 1 denotes Single Measure K denotes Average Measure
4. Discussion
DM is an irreversible chronic disease characterized by complex pathological mechanisms and numerous complications, one of the most significant being DCM. DCM is a myocardial structural and functional abnormality caused by diabetes itself, independent of coronary artery disease and hypertension
| [2] | Bhagyalakshmi, Balakrishnan, Raghu Chandrashekar, et al. Hyperglycaemia to heart failure: molecular pathophysiology, clinical manifestations, and novel therapeutic targets for diabetic cardiomyopathy. [J]. Arch Physiol Biochem, 2025, undefined: 1-14. https://doi.org/10.1080/13813455.2025.2567336 |
[2]
. Its pathogenesis primarily includes 1) metabolic disorders due to Insulin Resistance and Hyperglycemia: This leads to impaired glucose utilization by cardiomyocytes, accompanied by an excess of toxic intermediates (such as ceramide and reactive oxygen species), resulting in "lipotoxicity" those damages heart muscle cells. Furthermore, mitochondrial dysfunction reduces ATP production and generates large amounts of reactive oxygen species (ROS), triggering oxidative stress
. 2) Oxidative Stress: Excessive ROS attacks intracellular proteins, lipids, and DNA, directly causing cardiomyocyte damage, apoptosis, and necrosis
| [2] | Bhagyalakshmi, Balakrishnan, Raghu Chandrashekar, et al. Hyperglycaemia to heart failure: molecular pathophysiology, clinical manifestations, and novel therapeutic targets for diabetic cardiomyopathy. [J]. Arch Physiol Biochem, 2025, undefined: 1-14. https://doi.org/10.1080/13813455.2025.2567336 |
[2]
. 3) Accumulation of Advanced Glycation End Products (AGEs): In a persistent hyperglycemic environment, proteins and lipids undergo non-enzymatic glycation, forming AGEs. The binding of AGEs to their receptors activates pro-inflammatory and pro-fibrotic signaling pathways and causes "cross-linking" of collagen in the myocardial interstitium, increasing myocardial stiffness and impairing diastolic function
| [17] | Ilaria, Russo, Nikolaos G, et al. Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities. [J]. J Mol Cell Cardiol, 2015, 90: 84-93.
https://doi.org/10.1016/j.yjmcc.2015.12.011 |
[17]
. 4) Myocardial Fibrosis: Driven by inflammatory factors and growth factors, cardiac fibroblasts become overactive, producing excessive extracellular matrix (primarily collagen I and III), which replaces damaged cardiomyocytes. This leads to myocardial hypertrophy, stiffness, initial impairment of diastolic function, and subsequent progression to systolic dysfunction
| [4] | Mohapradeep, Mohan, Adel, et al. Left Ventricular Hypertrophy in Diabetic Cardiomyopathy: A Target for Intervention. [J]. Front Cardiovasc Med, 2021, 8: 746382.
https://doi.org/10.3389/fcvm.2021.746382 |
| [18] | Izabela, Tuleta, Nikolaos G, et al. Fibrosis of the diabetic heart: Clinical significance, molecular mechanisms, and therapeutic opportunities. [J]. Adv Drug Deliv Rev, 2021, 176: 113904.
https://doi.org/10.1016/j.addr.2021.113904 |
[4, 18]
. 5) Microvascular Disease: Hyperglycemia damages the endothelial cells of coronary microvessels, leading to impaired vasodilation, basement membrane thickening, and reduced capillary density. The consequence is decreased myocardial perfusion and chronic ischemia, particularly in areas with high oxygen demand
| [18] | Izabela, Tuleta, Nikolaos G, et al. Fibrosis of the diabetic heart: Clinical significance, molecular mechanisms, and therapeutic opportunities. [J]. Adv Drug Deliv Rev, 2021, 176: 113904.
https://doi.org/10.1016/j.addr.2021.113904 |
[18]
. 6) Cardiac Autonomic Neuropathy: Diabetes can also damage the autonomic nerves innervating the heart, leading to reduced heart rate variability, resting tachycardia, and impaired cardiac adaptation to load changes. Therefore, the early detection of cardiac functional changes in diabetes patients and proactive intervention are crucial for improving patient quality of life and survival rates
.
Currently, the ejection fraction (EF) is the primary clinical indicator used to assess cardiac function in diabetes patients. However, it has limited sensitivity for the early detection of myocardial impairment. Consequently, there is a need for more sensitive and objective parameters to evaluate and enable early intervention for incipient cardiac systolic dysfunction in diabetes patients. Left ventricular GLS, derived from two-dimensional speckle tracking echocardiography, has emerged as an objective early indicator. It is already applied for subclinical cardiac function assessment in various conditions with preserved EF, such as hypertension, nephrotic syndrome, valvular heart disease, and diabetes
| [7] | Victoria, Delgado, Nina, et al. Implementing Quality Control of LV Longitudinal Strain Measurement. [J]. JACC Cardiovasc Imaging, 2016, 10: 523-525.
https://doi.org/10.1016/j.jcmg.2016.09.003 |
| [20] | Christos G, Mihos, Jennifer E, et al. Speckle-Tracking Strain Echocardiography for the Assessment of Left Ventricular Structure and Function: A Scientific Statement From the American Heart Association. [J]. Circulation, 2025, 152: e96-e109. https://doi.org/10.1161/CIR.0000000000001354 |
[7, 20]
. Despite its utility, GLS may lack sufficient sensitivity and specificity for detecting the very earliest, most subtle myocardial injury or for localizing damage to specific myocardial layers
| [5] | Victor, Mor-Avi, Roberto M, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. [J].J Am Soc Echocardiogr, 2011, 24: 277-313. https://doi.org/10.1016/j.echo.2011.01.015 |
[5]
. This limitation led to the development of layered strain analysis, which aligns with the anatomical arrangement of the myocardium. The highly ordered, three-layered structure of the human left ventricle is the mechanical basis for its efficient pumping function: 1) subepicardial Layer: The myocardial fibers in this layer have a right-handed helical orientation (clockwise spiral from apex to base). They are primarily responsible for the heart's twisting motion. During systole, contraction of the subepicardium causes the apex to rotate counterclockwise (viewed from the apex) relative to the base, akin to "wringing a towel." This motion is crucial for rapid ejection. 2) Mid-myocardial Layer: The fibers in this, the thickest layer, are oriented circumferentially. They serve as the "main force," responsible for ventricular narrowing and thickening, generating significant radial force, and are the primary source of ventricular pressure and ejection. 3) Subendocardial Layer: The fibers in this layer have a left-handed helical orientation (counterclockwise spiral from apex to base). During diastole, contraction of the subendocardium aids in ventricular "untwisting," helping the heart return to its original shape to facilitate filling. It also contributes to longitudinal shortening. This triple-layered helical structure enables a complex mechanical process of twisting-narrowing-untwisting during left ventricular contraction. This design achieves highly efficient blood ejection with minimal energy expenditure. Among these layers, the subepicardial helical fibers may contribute most to the twisting function and are also the most sensitive to energy demands and oxygen supply. Layered strain analysis was developed to leverage this anatomical insight. It can more sensitively detect injury patterns within different myocardial layers in the early stages of disease, thereby hinting at distinct underlying pathophysiological mechanisms and providing deeper diagnostic clues
| [8] | Darae, Kim, Chi Young, et al. Differences in left ventricular functional adaptation to arterial stiffness and neurohormonal activation in patients with hypertension: a study with two-dimensional layer-specific speckle tracking echocardiography. [J]. Clin Hypertens, 2017, 23: 21.
https://doi.org/10.1186/s40885-017-0078-9 |
[8]
. For instance: In hypertrophic cardiomyopathy, while the GLS might be only mildly abnormal, the subendocardial longitudinal strain often shows a significant reduction, whereas the mid-myocardial and subepicardial strains may be relatively preserved or less impaired. In dilated cardiomyopathy, the longitudinal strain is typically significantly reduced across all three layers (subendocardial, mid-myocardial, and subepicardial), and the strain gradient (the difference between layers) is markedly diminished or absent
.
Our study found that compared to the control group, the case group showed elevated levels of glycated hemoglobin and systolic blood pressure. The increase in systolic blood pressure may be attributed to elevated extracellular glucose levels directly altering intracellular calcium concentration in cardiomyocytes. This leads to changes in myocardial contractile function, prolongs the time to peak contraction and repolarization, ultimately resulting in abnormal cardiac systolic function in diabetes patients. Furthermore, this study revealed that the case group had thickened interventricular septum compared to the control group. The potential mechanism is that activation of the renin-angiotensin-aldosterone system (RAAS) in diabetes patients causes local conversion of angiotensinogen to angiotensin II (Ang II) in the myocardium, triggering segmental and global cardiac remodeling. Concurrently, systemic metabolic disorders lead to the formation and deposition of advanced glycation end products and various lipid droplets, contributing to increased septal thickness and reduced compliance
| [21] | Loek, van Heerebeek, Nazha, et al. Diastolic stiffness of the failing diabetic heart: importance of fibrosis, advanced glycation end products, and myocyte resting tension. [J]. Circulation, 2007, 117: 43-51.
https://doi.org/10.1161/CIRCULATIONAHA.107.728550 |
| [22] | João Pedro Thimotheo, Batista, André Oliveira Vilela de, et al. The Role of Renin-Angiotensin System in Diabetic Cardiomyopathy: A Narrative Review. [J]. Life (Basel), 2023, 13.
https://doi.org/10.3390/life13071598 |
[21, 22]
. Notably, a significant increase in left ventricular posterior wall thickness was observed only in the left ventricular remodeling subgroup. This suggests that the impact of diabetes on the interventricular septum precedes its effect on the posterior wall. As metabolic disturbances worsen in diabetes patients, increased oxidative stress promotes the expression of pro-fibrotic and pro-inflammatory factors, ultimately leading to aggravated cardiac fibrosis
| [17] | Ilaria, Russo, Nikolaos G, et al. Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities. [J]. J Mol Cell Cardiol, 2015, 90: 84-93.
https://doi.org/10.1016/j.yjmcc.2015.12.011 |
| [21] | Loek, van Heerebeek, Nazha, et al. Diastolic stiffness of the failing diabetic heart: importance of fibrosis, advanced glycation end products, and myocyte resting tension. [J]. Circulation, 2007, 117: 43-51.
https://doi.org/10.1161/CIRCULATIONAHA.107.728550 |
[17, 21]
.
Results of left ventricular layered longitudinal strain in this study revealed that, compared to the control group, the case group exhibited significantly reduced absolute values of longitudinal strain in the subendocardial, mid-myocardial, and subepicardial layers of the three-chamber view; the subepicardial layer of the four-chamber view; and the average mid-myocardial and subepicardial strains. However, no statistically significant impairment was observed in the layered strain of the apical two-chamber view. This indicates that the impairment of left ventricular strain varies across the three standard apical views (three-chamber, two-chamber, and four-chamber) in diabetes patients, a finding potentially related to coronary blood supply. The three-chamber view is primarily supplied by the left anterior descending and left circumflex arteries, while the right coronary artery supplies several segments in the four-chamber view. Given that coronary lesions most commonly affect the left coronary artery, this differential blood supply may lead to varying degrees of myocardial damage in different left ventricular segments in DM, subsequently manifesting as view-specific differences in contractile function impairment. The observed reduction in the absolute values of subepicardial longitudinal strain (in the three-chamber and four-chamber views) and the average subepicardial strain in both the normal geometry and remodeling DM subgroups, compared to controls, may be attributed to several factors: 1) The subepicardial helical fibers are responsible for the high-energy-demand "twisting" motion, consuming significantly more oxygen per unit volume than the mid- or subendocardial layers, which may make them most vulnerable to damage. 2) Coronary blood flow progresses from the epicardium to the endocardium. The subepicardium, despite being "upstream," is most affected by intraventricular pressure. In the context of microvascular disease and diastolic dysfunction, the subepicardial blood flow reserve may be compromised first. Diabetes exacerbates this by reducing energy production efficiency (increased demand due to lipotoxicity and insulin resistance) while simultaneously decreasing oxygen supply (due to microvascular disease). This energy supply-demand mismatch is critical in the high-demand subepicardium, making it the first region to experience ischemia, hypoxia, and cellular injury. 3) Subtle injury in the subepicardium primarily may impacts cardiac twisting and untwisting, manifesting as reduced longitudinal strain and impaired torsion—an early sign of diastolic dysfunction, often evident in the heart failure with preserved ejection fraction (HFpEF) stage. 4) As DM progresses, subepicardial damage worsens and extends to the mid-myocardial layer, may affecting the circumferential fibers responsible for generating the primary ejection force. This leads to a decline in global systolic function and reduced ejection fraction, marking the progression to systolic dysfunction. 5) Fibrosis localization: Since the subepicardium may be the initial site of injury, interstitial fibrosis in DCM often starts here, further increasing stiffness in this region and impairing diastolic function. Furthermore, the reduction in the absolute values of strain in the subendocardial and mid-myocardial layers of the three-chamber view, and the subendocardial layer and average myocardial strain of the four-chamber view, was exclusively detected in the left ventricular remodeling subgroup. This is likely because patients in the DM with remodeling subgroup have been exposed to the hyperglycemic environment for a longer duration, exhibiting more pronounced myocardial hypertrophy, fibrosis, and altered left ventricular geometry. Concurrently, they likely have more extensive and severe concomitant coronary vascular disease, ultimately leading to more profound myocardial damage.
5. Conclusion
In summary, our findings demonstrate that left ventricular layered longitudinal strain can be utilized for the early assessment of impaired cardiac systolic function in patients with diabetes mellitus. More importantly, we observed that the presence or absence of left ventricular remodeling in diabetes patients differentially influences layered strain. In both the normal geometry and remodeling subgroups, impairment of longitudinal strain in the subepicardial layer (specifically in the three-chamber and four-chamber views) and in the average subepicardial strain manifested early. However, in the left ventricular remodeling subgroup, changes in the subendocardial and mid-myocardial layers of the three-chamber view, the subendocardial layer of the four-chamber view, and the average GLS exhibited the greatest sensitivity, indicating more advanced myocardial dysfunction.
6. Study Limitations
This study has the following limitations: Firstly, data collection was interrupted due to the COVID-19 pandemic, resulting in an insufficient sample size. Secondly, the lipid profile, renal function (eGFR/UACR), smoking status etc may be associate with LV strain and remodeling, those factors should be inclouded in future research. Thirdly, as a cross-sectional study, multiple comparisons and endpoints were lacking for explored the value of left ventricular layered longitudinal strain in assessing diabetes patients with or without left ventricular remodeling. Finally, given the complex and diverse mechanisms of diabetic myocardial injury, follow-up studies are necessary to further evaluate the significance of layered longitudinal strain in cardiovascular risk stratification and personalized management for diabetes patients.
Abbreviations
2DSTE | Two-dimensional Speckle Tracking Echocardiography |
LV | Left Ventricular |
DM | Diabetes Mellitus |
DCM | Diabetic Cardiomyopathy |
LVEF | Left Ventricular Ejection Fraction |
GLS | Global Longitudinal Strain |
RWT | Relative Wall Thickness |
LVEDD | Left Ventricular End-diastolic Diameter |
PWDD | Posterior Wall End-diastolic Diameter |
LVEDV | Left Ventricular End-diastolic Volume |
ECG | Electrocardiogram |
ICC | Intraclass Correlation Coefficient |
BSA | Body Surface Area |
ROS | Reactive Oxygen Species |
AGEs | Advanced Glycation End Products |
RAAS | Renin-angiotensin-aldosterone System |
IVST | Interventricular Septal Thickness |
Author Contributions
Kun Li: Data curation, Methodology, Writing – original draft
Jingqi Wang: Data curation, Project administration
Ling Liao: Data curation, Investigation
Chunmei Li: Conceptualization, Formal Analysis, Methodology, Writing – review & editing
Conflicts of Interest
The authors declare no competing interests.
References
| [1] |
Hong, Sun, Pouya, Saeedi, Suvi, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. [J]. Diabetes Res Clin Pract, 2021, 183: 109119.
https://doi.org/10.1016/j.diabres.2021.109119
|
| [2] |
Bhagyalakshmi, Balakrishnan, Raghu Chandrashekar, et al. Hyperglycaemia to heart failure: molecular pathophysiology, clinical manifestations, and novel therapeutic targets for diabetic cardiomyopathy. [J]. Arch Physiol Biochem, 2025, undefined: 1-14.
https://doi.org/10.1080/13813455.2025.2567336
|
| [3] |
W B, Kannel, M, et al. Role of diabetes in congestive heart failure: the Framingham study. [J]. Am J Cardiol, 1974, 34: 29-34.
https://doi.org/10.1016/0002-9149(74)90089-7
|
| [4] |
Mohapradeep, Mohan, Adel, et al. Left Ventricular Hypertrophy in Diabetic Cardiomyopathy: A Target for Intervention. [J]. Front Cardiovasc Med, 2021, 8: 746382.
https://doi.org/10.3389/fcvm.2021.746382
|
| [5] |
Victor, Mor-Avi, Roberto M, et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications endorsed by the Japanese Society of Echocardiography. [J].J Am Soc Echocardiogr, 2011, 24: 277-313.
https://doi.org/10.1016/j.echo.2011.01.015
|
| [6] |
Elizabeth, Potter, Thomas H, et al. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. [J]. JACC Cardiovasc Imaging, 2018, 11: 260-274.
https://doi.org/10.1016/j.jcmg.2017.11.017
|
| [7] |
Victoria, Delgado, Nina, et al. Implementing Quality Control of LV Longitudinal Strain Measurement. [J]. JACC Cardiovasc Imaging, 2016, 10: 523-525.
https://doi.org/10.1016/j.jcmg.2016.09.003
|
| [8] |
Darae, Kim, Chi Young, et al. Differences in left ventricular functional adaptation to arterial stiffness and neurohormonal activation in patients with hypertension: a study with two-dimensional layer-specific speckle tracking echocardiography. [J]. Clin Hypertens, 2017, 23: 21.
https://doi.org/10.1186/s40885-017-0078-9
|
| [9] |
Otto A, Smiseth, et al. Myocardial strain imaging: how useful is it in clinical decision making? [J]. Eur Heart J, 2015, 37: 1196-207.
https://doi.org/10.1093/eurheartj/ehv529
|
| [10] |
Patrick, Garceau, Shemy, et al. Evaluation of left ventricular relaxation and filling pressures in obstructive hypertrophic cardiomyopathy: comparison between invasive hemodynamics and two-dimensional speckle tracking. [J]. Echocardiography, 2012, 29: 934-42.
https://doi.org/10.1111/j.1540-8175.2012.01708.x
|
| [11] |
Ieva, Kažukauskienė, Giedrė, et al. Left ventricular global longitudinal strain predicts elevated cardiac pressures and poor clinical outcomes in patients with non-ischemic dilated cardiomyopathy. [J]. Cardiovasc Ultrasound, 2021, 19: 21.
https://doi.org/10.1186/s12947-021-00254-1
|
| [12] |
Wei-Ting, Chang, Wen-Huang, et al. Left ventricular global longitudinal strain is independently associated with mortality in septic shock patients. [J]. Intensive Care Med, 2015, 41: 1791-9.
https://doi.org/10.1007/s00134-015-3970-3
|
| [13] |
Despina-Manuela, Toader, Alina, et al. Layer-Specific Strain Analysis in Patients with Dilated Cardiomyopathy. [J]. Biomedicines, 2025, 13:
https://doi.org/10.3390/biomedicines13010011
|
| [14] |
Helmut, Baumgartner, Judy, et al. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. [J]. J Am Soc Echocardiogr, 2017, 30: 372-392.
https://doi.org/10.1016/j.echo.2017.02.009
|
| [15] |
Diagnosis and Classification of Diabetes: Standards of Care in Diabetes-2025. [J]. Diabetes Care, 2024, 48: S27-S49.
https://doi.org/10.2337/dc25-S002
|
| [16] |
Xudong, Zhao, Shengwang, et al. Diabetic cardiomyopathy: Clinical phenotype and practice. [J]. Front Endocrinol (Lausanne), 2022, 13: 1032268.
https://doi.org/10.3389/fendo.2022.1032268
|
| [17] |
Ilaria, Russo, Nikolaos G, et al. Diabetes-associated cardiac fibrosis: Cellular effectors, molecular mechanisms and therapeutic opportunities. [J]. J Mol Cell Cardiol, 2015, 90: 84-93.
https://doi.org/10.1016/j.yjmcc.2015.12.011
|
| [18] |
Izabela, Tuleta, Nikolaos G, et al. Fibrosis of the diabetic heart: Clinical significance, molecular mechanisms, and therapeutic opportunities. [J]. Adv Drug Deliv Rev, 2021, 176: 113904.
https://doi.org/10.1016/j.addr.2021.113904
|
| [19] |
Cardiovascular Disease and Risk Management: Standards of Care in Diabetes-2024. [J]. Diabetes Care, 2023, 47: S179-S218.
https://doi.org/10.2337/dc24-S010
|
| [20] |
Christos G, Mihos, Jennifer E, et al. Speckle-Tracking Strain Echocardiography for the Assessment of Left Ventricular Structure and Function: A Scientific Statement From the American Heart Association. [J]. Circulation, 2025, 152: e96-e109.
https://doi.org/10.1161/CIR.0000000000001354
|
| [21] |
Loek, van Heerebeek, Nazha, et al. Diastolic stiffness of the failing diabetic heart: importance of fibrosis, advanced glycation end products, and myocyte resting tension. [J]. Circulation, 2007, 117: 43-51.
https://doi.org/10.1161/CIRCULATIONAHA.107.728550
|
| [22] |
João Pedro Thimotheo, Batista, André Oliveira Vilela de, et al. The Role of Renin-Angiotensin System in Diabetic Cardiomyopathy: A Narrative Review. [J]. Life (Basel), 2023, 13.
https://doi.org/10.3390/life13071598
|
Cite This Article
-
APA Style
Li, K., Wang, J., Liao, L., Li, C. (2026). Value of Left Ventricular Layer-specific Strain in Detecting Left Ventricular Dysfunction in Diabetes Patients with Left Ventricular Remodeling and Non-remodeling. International Journal of Anesthesia and Clinical Medicine, 14(1), 21-30. https://doi.org/10.11648/j.ijacm.20261401.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Li, K.; Wang, J.; Liao, L.; Li, C. Value of Left Ventricular Layer-specific Strain in Detecting Left Ventricular Dysfunction in Diabetes Patients with Left Ventricular Remodeling and Non-remodeling. Int. J. Anesth. Clin. Med. 2026, 14(1), 21-30. doi: 10.11648/j.ijacm.20261401.14
Copy
|
Download
AMA Style
Li K, Wang J, Liao L, Li C. Value of Left Ventricular Layer-specific Strain in Detecting Left Ventricular Dysfunction in Diabetes Patients with Left Ventricular Remodeling and Non-remodeling. Int J Anesth Clin Med. 2026;14(1):21-30. doi: 10.11648/j.ijacm.20261401.14
Copy
|
Download
-
@article{10.11648/j.ijacm.20261401.14,
author = {Kun Li and Jingqi Wang and Ling Liao and Chunmei Li},
title = {Value of Left Ventricular Layer-specific Strain in Detecting Left Ventricular Dysfunction in Diabetes Patients with Left Ventricular Remodeling and Non-remodeling},
journal = {International Journal of Anesthesia and Clinical Medicine},
volume = {14},
number = {1},
pages = {21-30},
doi = {10.11648/j.ijacm.20261401.14},
url = {https://doi.org/10.11648/j.ijacm.20261401.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijacm.20261401.14},
abstract = {To explore the application of left ventricular (LV) stratified strain in evaluating early systolic dysfunction in diabetes patients with and without LV remodeling by using two-dimensional speckle tracking echocardiography (2DSTE), This study included 35 diabetes patients and 25 healthy individuals. All participants completed echography by GE Vivid E9 ultrasound system. The diabetes patients were subdivided based on relative wall thickness into normal LV geometry group and LV remodeling group. The EchoPAC offline workstation was used to analyze LV myocardial longitudinal layer-specific strain. Our results showed that compared to the control group, the absolute values of longitudinal strain in the endocardial, mid-myocardial, and epicardial layers of the 3-chamber view, the epicardial layer of the 4-chamber view, as well as the average longitudinal strain of the mid-myocardial and epicardial layers across all three views, were significantly decreased in the diabetes group (P < 0.05). Compared to the control group, both the normal LV geometry and LV remodeling subgroups showed significantly reduced absolute values of longitudinal strain in the epicardial layer of the 3-chamber and 4-chamber views, and in the average epicardial strain across all three views (P < 0.05), with the most pronounced changes observed in the LV remodeling group. Furthermore, compared to the control group, the LV remodeling subgroup exhibited significantly reduced absolute values of longitudinal strain in the endocardial and mid-myocardial layers of the 3-chamber view, the endocardial layer of the 4-chamber view, and the average mid-myocardial strain across all three views (P < 0.05). A significant decrease in the absolute value of epicardial longitudinal strain in the 3-chamber view was also found in the LV remodeling group compared to the normal LV geometry group (P < 0.05). The study reveals that in diabetes patients with either normal LV geometry or LV remodeling, impairment of epicardial longitudinal strain in the 3-chamber and 4-chamber views, as well as the average epicardial strain, occurs earlier. In diabetes patients with LV remodeling, longitudinal strain in the endocardial and mid-myocardial layers of the 3-chamber view, the endocardial layer of the 4-chamber view, and the average mid-myocardial strain were the most sensitively impaired parameters. Additionally, the impairment of myocardial longitudinal strain was most pronounced in the apical 3-chamber view.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Value of Left Ventricular Layer-specific Strain in Detecting Left Ventricular Dysfunction in Diabetes Patients with Left Ventricular Remodeling and Non-remodeling
AU - Kun Li
AU - Jingqi Wang
AU - Ling Liao
AU - Chunmei Li
Y1 - 2026/02/26
PY - 2026
N1 - https://doi.org/10.11648/j.ijacm.20261401.14
DO - 10.11648/j.ijacm.20261401.14
T2 - International Journal of Anesthesia and Clinical Medicine
JF - International Journal of Anesthesia and Clinical Medicine
JO - International Journal of Anesthesia and Clinical Medicine
SP - 21
EP - 30
PB - Science Publishing Group
SN - 2997-2698
UR - https://doi.org/10.11648/j.ijacm.20261401.14
AB - To explore the application of left ventricular (LV) stratified strain in evaluating early systolic dysfunction in diabetes patients with and without LV remodeling by using two-dimensional speckle tracking echocardiography (2DSTE), This study included 35 diabetes patients and 25 healthy individuals. All participants completed echography by GE Vivid E9 ultrasound system. The diabetes patients were subdivided based on relative wall thickness into normal LV geometry group and LV remodeling group. The EchoPAC offline workstation was used to analyze LV myocardial longitudinal layer-specific strain. Our results showed that compared to the control group, the absolute values of longitudinal strain in the endocardial, mid-myocardial, and epicardial layers of the 3-chamber view, the epicardial layer of the 4-chamber view, as well as the average longitudinal strain of the mid-myocardial and epicardial layers across all three views, were significantly decreased in the diabetes group (P < 0.05). Compared to the control group, both the normal LV geometry and LV remodeling subgroups showed significantly reduced absolute values of longitudinal strain in the epicardial layer of the 3-chamber and 4-chamber views, and in the average epicardial strain across all three views (P < 0.05), with the most pronounced changes observed in the LV remodeling group. Furthermore, compared to the control group, the LV remodeling subgroup exhibited significantly reduced absolute values of longitudinal strain in the endocardial and mid-myocardial layers of the 3-chamber view, the endocardial layer of the 4-chamber view, and the average mid-myocardial strain across all three views (P < 0.05). A significant decrease in the absolute value of epicardial longitudinal strain in the 3-chamber view was also found in the LV remodeling group compared to the normal LV geometry group (P < 0.05). The study reveals that in diabetes patients with either normal LV geometry or LV remodeling, impairment of epicardial longitudinal strain in the 3-chamber and 4-chamber views, as well as the average epicardial strain, occurs earlier. In diabetes patients with LV remodeling, longitudinal strain in the endocardial and mid-myocardial layers of the 3-chamber view, the endocardial layer of the 4-chamber view, and the average mid-myocardial strain were the most sensitively impaired parameters. Additionally, the impairment of myocardial longitudinal strain was most pronounced in the apical 3-chamber view.
VL - 14
IS - 1
ER -
Copy
|
Download